Osteoid Osteoma
G. Petur Nielsen, MD
Andrew E. Rosenberg, MD
Key Facts
Terminology
Benign bone-forming tumor characterized by its small size, limited growth potential, classic pattern of pain, and composition of woven bone trabeculae rimmed by osteoblasts
Clinical Issues
Accounts for approximately 13% of all primary benign bone tumors and 3% of all other primary bone tumors
Peak incidence: 5-25 years (76%)
Located in long tubular bones, especially lower extremity, followed by posterior elements of spine and tubular bones of hands and feet
Presents as severe localized pain that is often worse at night, which is relieved by aspirin or related medications
Induces joint pain that may mimic primary articular disorder
Most common cause of painful scoliosis
Treatment of choice is radiofrequency ablation with surgical removal in select patients
Excellent prognosis as lesion is not locally aggressive and does not metastasize
Image Findings
Does not exceed 1-2 cm in diameter
Lesion has well-defined margins and is round, lucent, and often contains variable amount of patchy central mineralization
Nidus is surrounded by zone of subperiosteal or medullary sclerosis
Increased uptake on bone scan
 Coronal T2-weighted MR of the right hip shows a case of an osteoid osteoma on the surface of the bone. The tumor is obscured by extensive intramedullary, periosteal, and soft tissue edema (bright white areas). |
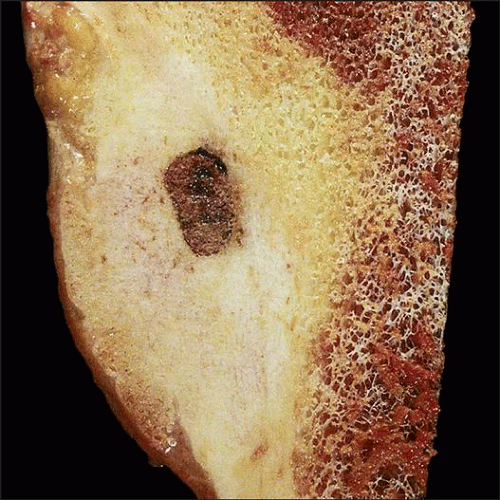 Resected subperiosteal osteoid osteoma is well demarcated from the surrounding thick subperiosteal reactive bone. The oval nidus is red-tan and does not involve the medullary cavity. |
TERMINOLOGY
Abbreviations
Osteoid osteoma (OO)
Definitions
Benign bone-forming tumor characterized by its small size, limited growth potential, classic pattern of pain, and composition of woven bone trabeculae rimmed by osteoblasts
CLINICAL ISSUES
Epidemiology
Incidence
Accounts for 13% of all primary benign bone tumors and 3% of all other primary bone tumors
Age
Usually develops in adolescents and young adults
Peak incidence: 5-25 years (76%)
Gender
Male predominance (2-3:1)
Site
Long tubular bones (75% of cases)
Proximal femur is most common location
Lesions are located in diaphysis and metaphysis (65-80%) and infrequently epiphysis
Common in subperiosteal region and within cortex (70-80%); intramedullary lesions less frequent (25%), intraarticular tumors are unusual
Vertebral column (10-14% of cases)
Posterior elements (90%), body (10%)
Short tubular bones of hands and feet (8-10%)
Presentation
Severe localized pain that is often worse at night, which is relieved by aspirin or other nonsteroidal anti-inflammatory medication
High levels of prostaglandin E2 and prostacyclins within nidus osteoblasts
COX-2 overexpression by osteoblasts
Joint pain mimicking that of primary articular disorder when lesion is located close to or within joints
Swelling that may mimic infection, especially when arising in small bones of hands and feet
Joint effusions
Painful scoliosis due to spasm of paravertebral muscles
Most common cause of painful scoliosis
Overgrowth of bone when located near growth plate
Limp and limitation of range of motion
Treatment
Radiofrequency ablation has become treatment of choice in most instances
Improves local control, eliminates removal of normal tissue, and is outpatient procedure
Curettage, burr down, or en bloc resection in cases that cannot be treated with radiofrequency ablation due to proximity to vital structures
Lesions located in spine frequently require surgical removal
Medical therapy and observation in selected patients
Prognosis
Excellent, as lesion is not locally aggressive and does not metastasize
Local recurrence rate following radiofrequency ablation is approximately 0-25%
IMAGE FINDINGS
General Features
Lesion (nidus) is 1-2 cm in diameter
Nidus has well-defined margins and often contains variable, patchy, central mineralization
Nidus surrounded by subperiosteal or medullary reactive sclerosis with adjacent soft tissue edema
Extensive reactive changes may simulate a more aggressive neoplasm and obscure lesion
Lesion is usually solitary and rarely multifocal
Radiographic Findings
Round, radiolucent with central mineralization
Peripheral sclerosis frequent and may be extensive
MR Findings
Isodense to skeletal muscle on T1-weighted images
Lucent components and surrounding edema have increased signal intensity on T2-weighted images
CT Findings
Well-demarcated, small, round lesion with central mineralization, bordered by reactive bone
Bone Scan
Marked uptake of radionuclide
MACROSCOPIC FEATURES
General Features
Tumor is round, well demarcated, gritty, dark red with central tan-white speckles and < 2 cm
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


