Patient Story
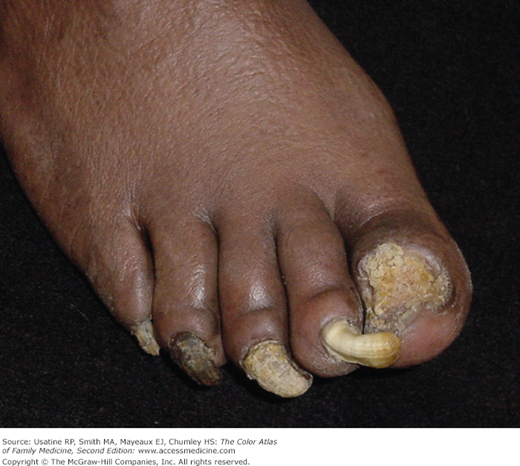
A 29-year-old woman presents with thickened and discolored toenails for 1 year (Figure 193-1). She is embarrassed to wear sandals and wants treatment. The entire nail plates are involved and there is subungual keratosis. She did not realize that she had tinea pedis, but a fine scale was seen on the soles and sides of the feet indicative of tinea pedis in a moccasin distribution. A KOH scraping from the subungual debris was positive for hyphae. She has no history of liver disease or risk factors for liver disease. An oral antifungal was prescribed for 3 months.

Introduction
Onychomycosis is a term used to denote nail infections caused by any fungus, including dermatophytes, yeasts, and nondermatophyte molds. One, some, and occasionally all of the toenails and/or fingernails may be involved. Although most toenail onychomycosis is caused by dermatophytes, many cases of fingernail onychomycosis are caused by yeast. Onychomycosis may involve the nail plate and other parts of the nail unit, including the nail matrix.
Epidemiology
- The incidence of onychomycosis has been reported to be 2% to 13% in North America.1
- Most patients (7.6%) only have toenail involvement and only 0.15% have fingernail involvement alone.2
- The prevalence of onychomycosis varies from 4% to 18%.3,4
- The disease is very common in adults, but may also occur in children.
Etiology and Pathophysiology
- Dermatophytes are responsible for most finger and toenail infections.
- Nonpathogenic fungi and Candida (in the rare syndrome of chronic mucocutaneous candidiasis) also can infect the nail plate (Figure 193-2).
- Dermatophytic onychomycosis (tinea unguium) occurs in three distinct forms: distal subungual, proximal subungual, and white superficial.
- The vast majority of distal and proximal subungual onychomycosis results from Trichophyton rubrum (Figure 193-3).
- White superficial onychomycosis is usually caused by Trichophyton mentagrophytes, although cases caused by T. rubrum have also been reported (Figure 193-4).
- Yeast onychomycosis is most common in the fingers caused by Candida albicans.



Risk Factors

Diagnosis
- Distal subungual onychomycosis is the most common presentation.
- Distal subungual onychomycosis begins with a whitish, yellowish, or brownish discoloration of a distal corner of the nail, which gradually spreads to involve the entire width of the nail plate and extends slowly toward the cuticle. Keratin debris collecting between the nail plate and its bed is the cause of the discoloration (Figures 193-1, 193-3, and 193-7).
- Proximal subungual onychomycosis progresses in a manner similar to distal subungual onychomycosis but affects the nail in the vicinity of the cuticle first and extends distally. It usually occurs in individuals with a severely compromised immune system (Figure 193-5).
- White superficial onychomycosis appears as dull white spots on the surface of the nail plate (Figure 193-4). Eventually the whole nail plate may be involved. The white areas may be soft and can be lightly scraped to yield a chalky scale that may be examined or cultured.

- Nail infection may occur in a single digit but most often occurs simultaneously in multiple digits of the foot. Toenails and fingernails may be affected at the same time especially in patients that are immunocompromised (Figures 193-5 and 193-6).



