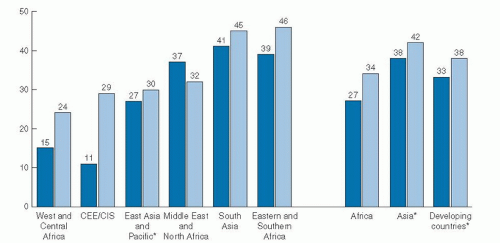
 Fig. 53.1. Trends globally, from 1995 to 2008, in the percentage of infants less than 6 months who were exclusively breast-fed. Asterisks, excluding China; CEE/CIS, Central and Eastern Europe/Commonwealth of Independent States region. (Data from UNICEF. UNICEF Global Databases 2010, from Multiple Indicator Cluster Surveys, Demographic Health Surveys, and Other National Surveys. Available at: http://www.childinfo.org/ breastfeeding_progress.html. Accessed June 28, 2011, with permission.) |
breast-feeding and 6-month breast-feeding were more common among white and Hispanic women than among black women (11). In the 2005 to 2006 birth cohort group, 65% of non-Hispanic black infants were breast-fed compared with 80% of Mexican-American and 79% of non-Hispanic white infants.
TABLE 53.1 IN-HOSPITAL AND 6-MONTH BREASTFEEDING RATES ACCORDING TO PARTICIPATION IN THE SPECIAL SUPPLEMENTAL NUTRITION PROGRAM FOR WOMEN, INFANTS, AND CHILDREN | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
For example, lactose increases; sodium, potassium, and chloride decrease; total lipids increase; the immune factors lactoferrin and secretory immunoglobulin A decrease; and oligosaccharides decrease. Representative values for early and mature human milk constituents are listed in Table 53.2 (18). Both the composition and volume of human milk secreted are influenced to some degree by factors such as genetic individuality, maternal intake (particularly fatty acids, vitamin B12, thiamin, riboflavin, vitamin B6, vitamin A, selenium, and iodine), and stage of lactation (19, 20, 21, 22, 23).
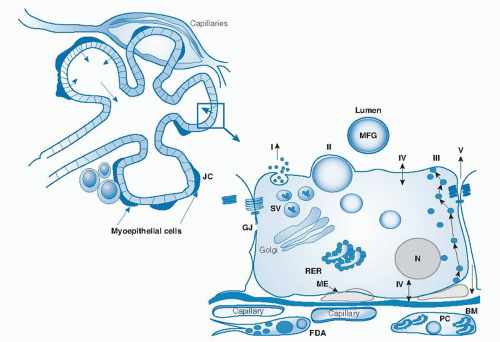 Fig. 53.2. Diagram of the mammary alveolus and alveolar epithelial cell showing pathways for milk secretion. Milk is secreted by alveolar epithelial cells into the lumen and is then expressed through the ducts by contraction of myoepithelial cells (ME). The alveolus is surrounded by a well-developed vasculature and a stroma that includes extracellular matrix components, fibroblasts, and adipocytes. The region inside the box is expanded to show key structural and transport properties of alveolar cells. I, Exocytotic secretion of milk proteins, lactose, calcium, and other aqueous-phase milk components. II, Formation of cytoplasmic lipid droplets that move to the apical membrane to be secreted as a membrane-bound milk fat globule (MFG). III, Vesicular transcytosis of proteins such as immunoglobulins from the interstitial space. IV, Transporters for the movement of monovalent ions, water, and glucose across the apical and basal membranes of the cell. V, Transport of plasma components and leukocytes through the paracellular pathway (open only during pregnancy, involution, and in inflammatory states such as mastitis). BM, basement membrane; FDA, fat-depleted adipocyte; GJ, gap junction; JC, junctional complex; N, nucleus; PC, plasma cell; RER, rough endoplasmic reticulum; SV, secretory vesicle. (Redrawn from McManaman JL, Neville MC. Mammary physiology and milk secretion. Adv Drug Del Rev 2003;55:629-41, with permission.) |
fraction of human milk comprises more than 200 compounds, including free amino acids, carnitine, taurine, amino sugars, nucleic acids, nucleotides, and polyamines. Maternal nutrition may alter both the total protein and nonprotein nitrogen constituents of human milk; however, healthy full-term exclusively breast-fed infants do not, as a rule, show signs of protein deficiency, regardless of maternal intake (22).
TABLE 53.2 REPRESENTATIVE VALUES FOR CONSTITUENTS OF HUMAN MILK | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


