Patient Story
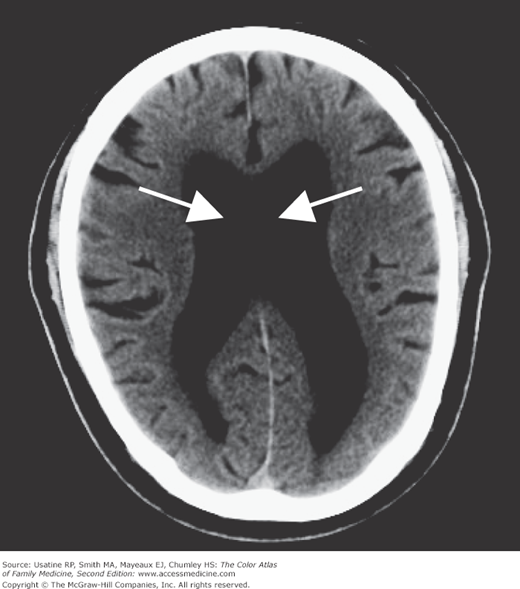
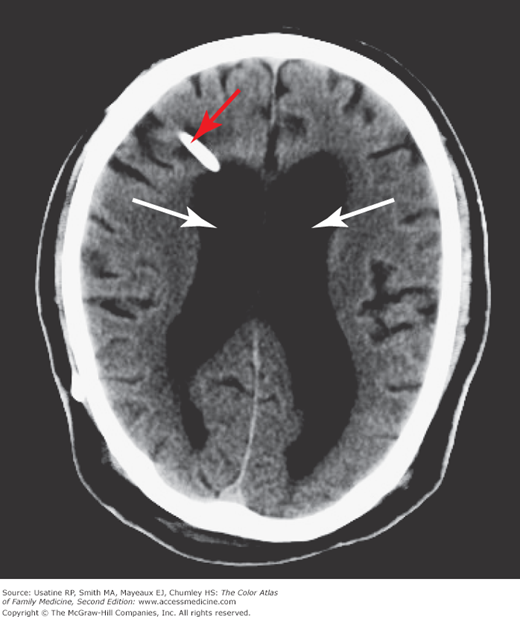
A 68-year-old man presented with a gradual onset of difficulty with his gait, increased urinary incontinence, and difficulty with his memory during the past several months. His gait was wide-based and slow, with decreased step height and length. His Mini Mental State Examination was consistent with impaired cognition. As part of his workup, he had a noncontrast head CT, which demonstrated dilated ventricles (Figure 232-1) without extensive cortical atrophy. He had normal cell counts and opening pressure on a spinal tap. He was diagnosed with normal pressure hydrocephalus (NPH) and referred to a neurosurgeon to be evaluated for a ventricular shunt. The patient had the shunt placed (Figure 232-2). His gait and urinary incontinence improved. Unfortunately, his cognitive impairments did not improve as is often the case.
Introduction
NPH can be idiopathic or secondary to meningitis, subarachnoid hemorrhage, or head trauma, and is caused by impaired reabsorption of spinal fluid. Patients present with gait abnormalities, urinary incontinence, and/or cognitive impairment. Diagnosis is confirmed by radiographic evidence and a normal opening pressure on lumbar puncture.
Epidemiology
Etiology and Pathophysiology
- Cerebral spinal fluid (CSF) is produced by the choroid plexus, circulates through the ventricles, exits into the subarachnoid space, and is reabsorbed by the arachnoid granulations at the top of the brain.3
- NPH is thought to be due to impaired reabsorption and can be idiopathic or secondary to meningitis, subarachnoid hemorrhage, or head trauma.
Diagnosis
NPH is a clinical diagnosis based on signs and symptoms, CSF studies, radiographic imaging, and a clinical response to ventriculoperitoneal (VP) shunting.
Classic triad is gait disturbance, urinary incontinence, and cognitive impairment:
- Gait disturbances typically occur first—Wide-based stance; slow, shuffling steps; difficulty with initiation.3
- Urinary incontinence usually with urgency; abnormal detrusor contractions on urodynamic studies.3
- Cognitive impairment—Difficulty with attention and concentration (digit span, arithmetic) with sparing of orientation and general memory.4
- CSF had normal cell counts and opening pressure less than 200 mm Hg.3

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


