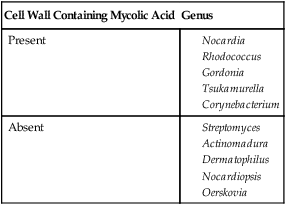
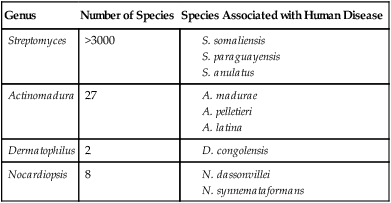
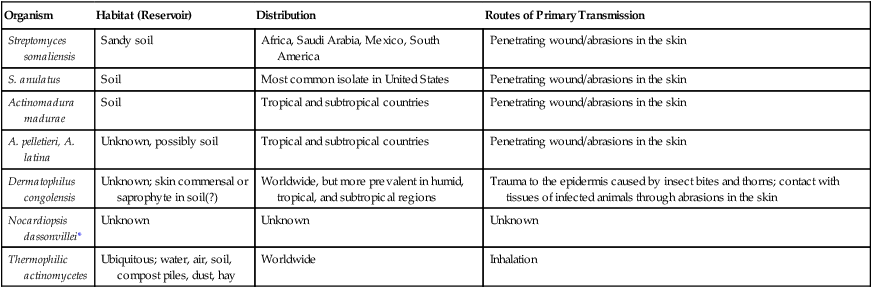
1. Describe the general characteristics of the aerobic actinomycetes, including their Gram stain morphology, microscopic morphology, colonial morphology, and biochemical reactions. 2. Describe the habitats of actinomycetes and the routes of transmission. 3. Describe the three types of skin infections caused by Nocardia spp. in immunocompromised individuals. 4. List the laboratory tests used to differentiate the clinically relevant aerobic actinomycetes. 5. List the laboratory tests used to differentiate the pathogenic Nocardia spp. 6. Describe the chemical structures required for an organism to be classified as acid-fast. 7. List the virulence factors associated with Nocardia asteroides. 8. Define mycetoma and actinomycetoma. 9. List the various selective media used to isolate aerobic actinomycetes and describe their usefulness in achieving optimal recovery. These organisms are aerobic, facultatively anaerobic, or obligately anaerobic; only the aerobic actinomycetes are discussed in this chapter. Aerobic actinomycetes belong to the order Actinomycetales. Actinomycetes comprise more than 40 genera, but only the clinically relevant aerobic actinomycetes genera are considered here (Table 19-1). In this chapter, only aerobic actinomycetes that exhibit branching and/or partial acid-fastness are addressed. Although both the Corynebacterium and Mycobacterium genera belong to the order Actinomycetales, Corynebacterium spp. do not usually exhibit branching filaments or partial acid-fastness, and Mycobacterium spp. do not exhibit branching and are strongly (acid-alcohol) acid-fast; for these reasons, the Corynebacteriaceae and Mycobacteriaceae are addressed in Chapters 17 and 43, respectively. Another clinically significant aerobic actinomycete is Tropheryma whipplei; because this organism has not been cultured on artificial media, it is reviewed in Chapter 44. For purposes of discussion, the remaining genera of aerobic actinomycetes are divided into the two large groups: those with cell walls that contain mycolic acid and are therefore partially acid-fast and those with cell envelopes that do not contain mycolic acid and therefore are non–acid-fast. TABLE 19-1 Clinically Relevant Aerobic Actinomycetes* *The genera Williamsia, Skermania, and Dietzia are also aerobic actinomycetes but to date are not clinically relevant. Currently, the taxonomy in the genus Nocardia is changing rapidly. Recognition and description of new species continue and remain controversial regarding the number of validly described species; recent publications cite 22 to 30 valid species. Of significance, Cloud et al.1 reported that the most commonly identified species was Nocardia cyriacigeorgica, not N. asteroides, as determined by partial 16S rRNA DNA sequencing, followed by N. farcinica, N. nova, N. africana, and N. veterana. The species considered human pathogens or that have been implicated as human pathogens are listed in Box 19-1. N. asteroides, N. nova, N. farcinica, N. brasiliensis, N. otitidiscaviarum (formerly N. caviae), N. pseudobrasiliensis, and N. transvalensis account for most of the diseases in humans caused by Nocardia spp. Organisms belonging to the Rhodococcus, Gordonia, and Tsukamurella genera are similar to Nocardia spp. in that they are gram-positive, aerobic, catalase-positive, partially acid-fast, branching, filamentous bacteria that can fragment into rods and cocci. The extent of acid-fastness depends on the amount and complexity of mycolic acids in the organism’s cell envelope and on culture conditions. The differentiation of these three genera, as well as species identification, is difficult. In particular, the genus Rhodococcus consists of a very diverse group of organisms in terms of morphology, biochemical characteristics, and ability to cause disease. As previously mentioned, the taxonomy of these organisms continues to evolve; species included in these three genera, as of this writing, are summarized in Table 19-2. TABLE 19-2 Species Included in the Genera Rhodococcus, Gordonia, and Tsukamurella Data compiled from Brown JM et al: In Murray PR, Baron EJ, Pfaller MA et al, editors: Manual of clinical microbiology, ed 10, Washington, DC, 2003, American Society for Microbiology; Goodfellow M, Chun J, Stubbs S et al: Lett Appl Microbiol 19:401, 1994; Klatte S, Rainey FA, Kroppenstedt RM: Int J Syst Bacteriol 44:769, 1994; Lasker BA, Brown JM, McNeil MM: Clin Infect Dis 15:233, 1992; Maertens J et al: Clin Microbiol Infect 4:51, 1998; Riegel P et al: J Clin Microbiol 34:2045, 1996; Yassin AF, Rainey FA, Burrghardt J et al: Int J Syst Bacteriol 47:607, 1997; Arenskötter M et al: Appl Environ Microbiol 70:3195, 2004 The non–acid-fast aerobic actinomycetes (i.e., Streptomyces, Actinomadura, Dermatophilus, Nocardiopsis, and the thermophilic actinomycetes) are gram-positive, branching filaments that do not contain mycolic acids in their cell envelopes and are therefore non–acid-fast. This group of actinomycetes is heterogeneous and is encountered infrequently in the clinical laboratory. Only the non–acid-fast actinomycetes associated with human disease are addressed (Table 19-3). TABLE 19-3 Non–Acid-Fast Aerobic Actinomycetes Associated with Human Disease Aspects of the epidemiology of the non–acid-fast aerobic actinomycetes are summarized in Table 19-4. Little is known about how these agents cause infection. TABLE 19-4 Epidemiology of the Non–Acid-Fast Aerobic Actinomycetes *Only a few cases of infection identified in the literature. The partially acid-fast actinomycetes cause various infections in humans. The types of infections caused by Rhodococcus, Gordonia, and Tsukamurella spp. are listed in Table 19-5. For the most part, these organisms are considered opportunistic pathogens, because most infections occur in immunocompromised individuals. TABLE 19-5 Infections Caused by Rhodococcus, Gordonia, and Tsukamurella spp. Pulmonary infections (pneumonia, lung abscess, pulmonary nodules) Skin, urinary tract, and wound infections Abscesses: prostatic/splenic, thyroid, renal, brain, subcutaneous
Nocardia, Streptomyces, Rhodococcus, and Similar Organisms
Cell Wall Containing Mycolic Acid
Genus
Present
Absent
General Characteristics
Partially Acid-Fast Aerobic Actinomycetes
Nocardia spp.
Rhodococcus, Gordonia, Tsukamurella spp.
Genus
Species
Rhodococcus
equi, erythropolis, rhodnii, rhodochrous (other species of unknown significance include globerulus, marinonascens, and ruber)
Gordonia
aichiensis, bronchialis, polyisoprenivorans, rubripertincta, sputi, terrae (remaining species isolated from environmental sources)
Tsukamurella
paurometabola, pulmonis, tyrosinosolvens, strandjordae (T. ichonensis, T. wratislaviensis isolated from nature)
Non–acid-Fast Aerobic Actinomycetes: Streptomyces, Actinomadura, Dermatophilus, Nocardiopsis, and the Thermophilic Actinomycetes
Genus
Number of Species
Species Associated with Human Disease
Streptomyces
>3000
Actinomadura
27
Dermatophilus
2
Nocardiopsis
8
Epidemiology and Pathogenesis
Partially Acid-Fast Aerobic Actinomycetes
Nocardia spp.
Non–acid-Fast Aerobic Actinomycetes: Streptomyces, Actinomadura, Dermatophilus, Nocardiopsis, and the Thermophilic Actinomycetes
Organism
Habitat (Reservoir)
Distribution
Routes of Primary Transmission
Streptomyces somaliensis
Sandy soil
Africa, Saudi Arabia, Mexico, South America
Penetrating wound/abrasions in the skin
S. anulatus
Soil
Most common isolate in United States
Penetrating wound/abrasions in the skin
Actinomadura madurae
Soil
Tropical and subtropical countries
Penetrating wound/abrasions in the skin
A. pelletieri, A. latina
Unknown, possibly soil
Tropical and subtropical countries
Penetrating wound/abrasions in the skin
Dermatophilus congolensis
Unknown; skin commensal or saprophyte in soil(?)
Worldwide, but more prevalent in humid, tropical, and subtropical regions
Trauma to the epidermis caused by insect bites and thorns; contact with tissues of infected animals through abrasions in the skin
Nocardiopsis dassonvillei*
Unknown
Unknown
Unknown
Thermophilic actinomycetes
Ubiquitous; water, air, soil, compost piles, dust, hay
Worldwide
Inhalation
Spectrum of Disease
Partially Acid-Fast Aerobic Actinomycetes
Rhodococcus, Gordonia, Tsukamurella spp.
Organism
Clinical Manifestations
Rhodococcus spp.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
