Fig. 18.1
In normal urothelium and in reactive atypia CK20 expression is limited to the umbrella cell layer (a); CD44 stains predominantly the basal cell layer, although patchy positivity can be seen in all layers (b)
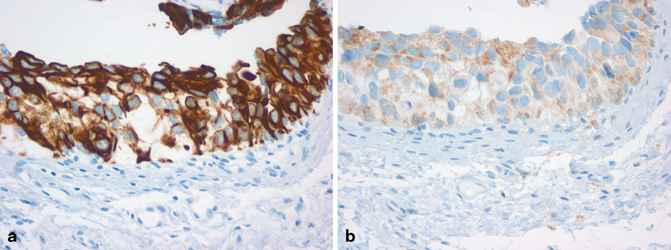
Fig. 18.2
Urothelial carcinoma in situ is expresses CK20 in the majority of tumor cells (full thickness) (a), with loss of CD44 expression (b)
It is important to note that none of these markers should be used individually to establish a malignant or benign diagnosis. Aberrant expression of these markers is well established and their interpretation must be made in the correct context. Moreover, IHC should not be used in all cases as a screening test, but rather as an adjunctive tool to aid in the histological classification of atypical flat urothelial lesions or in the de novo diagnosis of CIS where the morphologic features are questionable.
Differentiating Urothelial Carcinoma (with or Without Divergent Differentiation) from Other Carcinomas that Secondarily Involve the Urinary Bladder
Distinguishing invasive urothelial carcinoma from carcinomas secondarily involving the urinary bladder is of paramount significance and can at times be difficult due to significant morphologic overlap. Prostatic adenocarcinoma, colorectal adenocarcinoma, squamous cell carcinoma of the uterine cervix, and to a lesser extent, carcinomas of the uterus or ovary, and rarely those from breast, lung, stomach, and skin [5, 6], can involve the bladder during their course and may present a diagnostic challenge primarily in the absence of a relevant clinical history regarding the potential primary site of origin.
It is important to keep in mind that both squamous and glandular differentiations are common findings in primary urothelial carcinoma of the bladder but the diagnostic dilemmas can arise in cases of pure adenocarcinoma or squamous cell carcinoma involving the bladder. The best way to solve any potential misdiagnosis is to think of the possibility that these tumors can present in the bladder and to explore the clinical situation of the patient. Having a similar tumor in a site where it is more common to have tumors with the given morphology is perhaps the strongest clue favoring a metastatic origin of the bladder tumor.
Poorly Differentiated Prostatic Adenocarcinoma Versus Urothelial Carcinoma
These two entities might have morphologic overlap and the clinical management implications are significant. The history of prostatic adenocarcinoma might not be provided or might be overlooked. Additionally, some of these patients might have received treatments that affected the morphological appearance of the prostate cancer, further complicating its recognition.
Generally, a panel of markers is useful in separating the two entities in the majority of the cases. Markers that are supportive of prostatic differentiation (Fig. 18.3a) include prostate-specific antigen (PSA) (Fig. 18.3b), prostate-specific acid phosphatase (PSAP), prostate-specific membrane antigen (PSMA), P501s (Fig. 18.3c), NKX3.1 (Fig. 18.3d), and erythroblast transformation-specific-related gene (ERG); whereas, markers favoring urothelial differentiation (Fig. 18.4a) and origin include high molecular weight cytokeratin (34βe12), CK7 (Fig. 18.4b), p63 (Fig. 18.4c), thrombomodulin, uroplakin III, and recently GATA3 (Fig. 18.4d) [7–12].
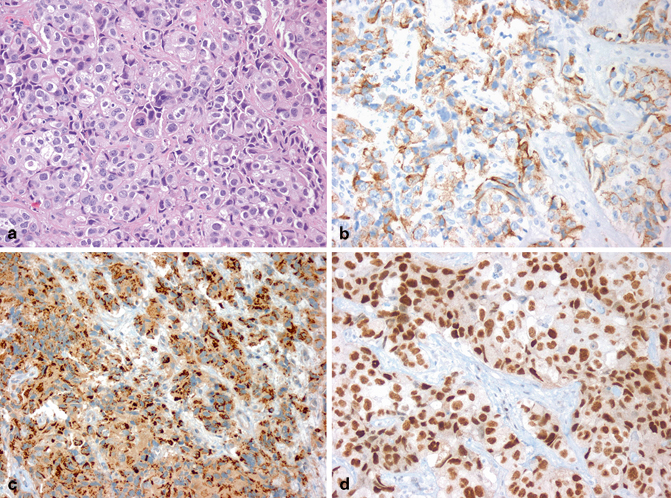
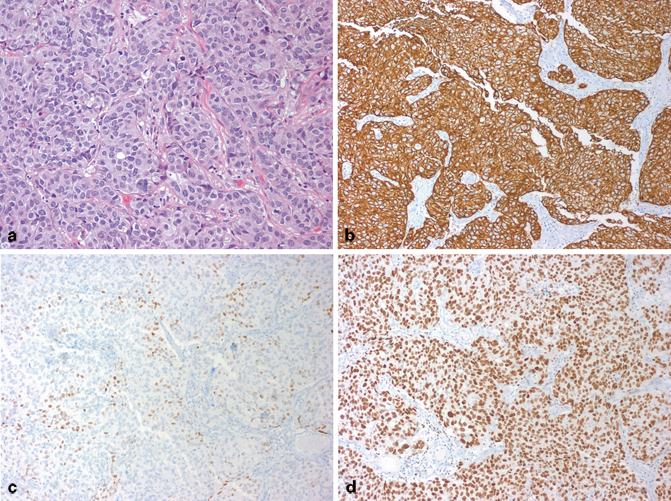
Fig. 18.3
Bladder neck tumor from a 70-year-old man with urine cytology positive for urothelial carcinoma (a). Tumor cells are positive for PSA (b), P501s (c), and NKX3.1 (d), supporting the diagnosis of prostatic adenocarcinoma
Fig. 18.4
Bladder mass from a 67-year-old man with urine cytology positive for urothelial carcinoma (a). Tumor is diffusely positive for CK7 (b), focally positive for p63 (c), and diffusely positive for GATA3 (d), supporting the diagnosis of urothelial carcinoma
Obviously not all of these markers are needed in any individual case. It is recommended to start with a few markers with high sensitivity and specificity and then use additional markers as needed. PSA, CK34βe12, and p63 are very useful as a start in the majority of cases.
A unique scenario is the presence of prostatic adenocarcinoma with extensive squamous differentiation involving the bladder. This is a rare situation that occurs primarily postradiation or hormone therapy for prostate cancer. The clues to the prostatic origin of such a tumor is the clinical suspicious based on the clinical history which should prompt careful and extensive examination of the tumor to find even the slightest glandular differentiation, which would then be confirmed by any of the prostatic markers mentioned above. It is only logical to keep in mind that these prostatic markers will not be expressed in the component with pure squamous differentiation.
Colorectal Adenocarcinoma Involving the Bladder by Direct Extension or Metastasis Versus Primary Bladder Adenocarcinoma (Enteric Morphology)
For this differential diagnosis, the clinical history is also extremely important which should include knowledge of the presence of a prior or current tumor of the colorectal region, its grade, and stage. These tumors may even colonize the bladder mucosa giving the impression of a “precursor” or “in situ” lesion. Unfortunately, IHC currently is of limited value in this differential diagnosis as tumors with enteric phenotype will generally stain similarly regardless of the site of origin. There have been suggestions that β-catenin might be of value in this scenario as it will not label the nuclei of primary bladder adenocarcinoma compared to those originating from the colorectal region [13–16]. While this pattern seems to be of value, nuclear localization of β-catenin was still reported in cases of primary bladder adenocarcinoma in some of these studies. Moreover, nuclear localization of β-catenin is not universal to all cases of primary colorectal adenocarcinoma, and a negative stain (i.e., only membranous and or cytoplasmic expression) will not exclude a colorectal primary. It is therefore, very important to always inquire about the clinical history of the patient for the possibility of a primary in the colorectal region when facing the diagnosis of enteric adenocarcinoma in the urinary bladder.
Squamous Cell Carcinoma of Uterine Cervix Involving the Bladder by Direct Extension or Metastasis Versus Primary Squamous Cell Carcinoma of the Bladder (or Urothelial Carcinoma with Squamous Differentiation)
Bladder involvement by squamous cell carcinoma of uterine cervical origin is admittedly rare but can still be diagnostically challenging when encountered, especially considering that squamous differentiation is rather common in urothelial carcinoma.
A number of markers have shown strong correlation with squamous neoplasms but unfortunately, these markers will not be able to point to a specific site of origin for these squamous carcinomas. Examples of such markers include desmogelin-3, MAC387, and TRIM29, which although sensitive markers for squamous phenotype, can be positive in squamous cell carcinoma of the cervix as well as that of the bladder. These markers can also be expressed in the squamous component of urothelial carcinoma with squamous differentiation and less commonly within the classical urothelial component [17, 18]. This is why these markers are not reliable as the sole means of establishing a site of origin for a tumor with squamous differentiation.
The role of the human papillomavirus (HPV) is well established in the vast majority of cervical squamous cell carcinoma for which p16 serves as a surrogate marker for the detection of HPV in these tumors [19, 20]. The expression of p16 in squamous cell carcinoma of the bladder has been shown to be less specific with little if any association with HPV infection in such setting [21]. There were, however, rare cases of true HPV-associated squamous cell carcinoma of the bladder and at least in some of them the tumors exhibited basaloid morphology and were associated with a history of neurogenic bladder or other situations that required repeated catheterization of the bladder [22, 23].
A number of other carcinomas may rarely involve the bladder during their course such as mammary carcinoma, endometrial or ovarian carcinoma, gastric carcinoma, etc. It is prudent to review the primary tumor alongside the metastasis. Immunostains might be ordered according to the suspected primary tumor, particularly if the status of such markers is known in the primary site.
Markers for the Differential Diagnosis of Spindle Cell Lesions of the Bladder
Many entities exist in the bladder in which spindle cell morphology predominates and range from reactive myofibroblastic lesions to frankly malignant (sarcomatous) entities. The main categories include inflammatory myofibroblastic tumor/pseudosarcomatous myofibroblastic proliferations (IMT/PMP), sarcomatoid urothelial carcinoma, and sarcomas with spindle cell morphology (leiomyosarcoma, rhabdomyosarcoma). There is marked overlap in morphology and immunoprofile among these entities and a judicious use of IHC in the context of morphology plays an important supportive role in this differential diagnosis.
Establishing the diagnosis of IMT can be aided by the expression of ALK by IHC or the presence of ALK rearrangement by fluorescence in situ hybridization (FISH) or other molecular technique . Since this expression or rearrangement is not present in all cases, a negative test does not rule out the diagnosis of IMT [24]. The overall morphologic features and the expression of other markers such as smooth muscle actin and cytokeratins may help. The challenge remains to differentiate this entity from a reactive myofibroblastic proliferation, which can be exuberant in the bladder.
For sarcomatoid urothelial carcinoma, finding an unequivocal epithelial component would be the ideal scenario but when this is not feasible, the presence of epithelial differentiation by IHC might be helpful in pointing toward the diagnosis of sarcomatoid UC. This can be achieved by a number of epithelial markers such as wide spectrum cytokeratins (AE1/AE3, CAM5.2…), epithelial membrane antigen (EMA), high molecular weight keratins, and p63. GATA3 might be helpful as well but we still do not know its full functions in spindle cell lesions in general and more studies are needed to assess its value in this setting.
For true sarcomas with specific lineage or differentiation such as leiomyosarcoma and rhabdomyosarcoma, the diagnosis can be confirmed by the markers related to these entities such as actin, desmin, myogenin, etc.
The Confirmation of Urothelial Differentiation at a Metastatic Site
Generally, urothelial carcinoma presents at metastatic sites with the morphology of a poorly differentiated carcinoma without specific morphologic features. It could be particularly difficult to distinguish metastatic urothelial carcinoma from metastatic squamous cell carcinoma (or from primary squamous cell carcinoma in the example of a lung tumor). What might be helpful in pointing to an origin of a urothelial primary include (1) prior history of bladder cancer, which should warrant review of the primary tumor if available and (2) the presence of divergent differentiation (squamous, glandular, etc.).
In these settings, IHC can play a role in establishing the urothelial origin of such tumors.
Antibodies that can be used to confirm urothelial differentiation/origin include GATA3, cytokeratins 7 and 20, high molecular weight cytokeratin, p63, uroplakin III, thrombomodulin, cytokeratin CK5/6, and S100P [25–28].
It is important to keep in mind that, despite their relative specific pattern of expressions, none of these markers is by itself diagnostic of a primary urothelial carcinoma as certain degree of overlap still exists and it may take more than one marker to help in this differential.
The Role of IHC in Confirming the Presence of Lymphovascular Invasion (LVI)
LVI in urothelial carcinoma has been reported to be an independent prognostic factor for metastasis, recurrence, and survival [29–31]. Identifying LVI, however, can be complicated by the presence of peri-tumoral stromal retraction, which is a relatively common finding in invasive urothelial carcinoma that mimics LVI. This is particularly problematic within the lamina propria. As a result, assessing LVI suffers from a considerable lack of diagnostic reproducibility, which limits its utility as a prognostic finding [32, 33]. If LVI is to retain its clinical significance, it should be reported with caution and after applying rigid criteria for its identification. In this regard, a number of endothelial/vascular IHC markers can be used to confirm the presence of LVI such as CD31, CD34, D2-40, and ERG [34, 35]. It is not recommended, however, to use these markers as a screening tool in all cases of invasive urothelial carcinoma and they should be used only in histologically equivocal cases for confirmation.
The Role of IHC in Staging of Bladder Cancer
For the majority of cases, documenting invasion in bladder cancer is not problematic by following well-established and recognized criteria [36]. In cases of ambiguity, however, such as thermal artifact, marked inflammation, or disrupted anatomy due to a prior biopsy, applying IHC may be helpful. The most commonly used markers are cytokeratins (AE1/AE3, CK7, CK8/18). An important caveat is the potential staining of stromal myofibroblasts with such epithelial markers.
Documenting tumor invasion of the muscularis propria (MP) is an important parameter in staging urothelial carcinoma, upon which major management decisions depend, such as proceeding to radical cystectomy or the administration of neoadjuvant chemotherapy. The distinction between MP and muscularis mucosae (MM) , although readily achieved by light microscopy in most cases, may be challenging in some situations, such as extensive tumor infiltration of tissue fragments, post-biopsy changes that mask the normal anatomy, marked thermal artifact of tumor-bearing tissue, or hyperplastic MM. Several muscle markers have been tried in the past but were found to be of limited utility such as smooth muscle actin, desmin, and caldesmon. Recent reports have identified a new marker, smoothelin, expressed by terminally differentiated smooth muscle cells, to be differentially expressed in smooth muscle of the MP compared to that of the MM [37–41]. It should be noted, however, that other studies reported overlap of staining intensity of smoothelin between MM and MP [42]. Hence, it is still early to determine the exact role of smoothelin as a diagnostic marker to determine tumor invasion into MP and should be used with caution.
Immunohistochemical Markers with Prognostic Value in Bladder Cancer
In papillary urothelial tumors , a number of markers have shown promising results, particularly in distinguishing between low-grade and high-grade papillary urothelial carcinoma and decreasing the interobserver variability in this category. Ki-67 and survivin were two markers that have been frequently studied and whose increased expression correlates with recurrence and progression of papillary tumors [43, 44]. Similar results were reported when the mRNA levels of survivin were measured both in urine cytology and tumor tissue [43, 45–48].
Despite the great advancement in the molecular biology of urothelial carcinoma, there has not been to date a molecular marker that outperforms a combination of established morphologic and clinical markers such as grade, histologic type, and stage, in predicting clinical outcome. This has been the case with the tumor suppressor genes p53 and Rb, which are known to be involved in urothelial neoplasia. Although they have been shown by several investigators to be accurate predictors of progression, metastasis, survival, and possibly response to systemic chemotherapy [49–53], others have challenged these results which have not been validated prospectively.
On the other hand, IHC can serve as a surrogate marker for underlying molecular aberrations that can be used in targeted therapy. In particular, alterations in receptor tyrosine kinases present promising opportunities for targeted therapy in urothelial carcinomas, such as those targeting ERBB2 (Her2) amplifications or mutations and FGFR3 mutations; as well as aberrations in the mTOR/Akt/PI3K pathway that are known to affect subsets of urothelial carcinoma [54–57].
GATA3 is a transcription factor of the GATA family whose functions include regulating genes involved in the luminal differentiation of breast epithelium, genes related to T-cell development, gene regulation in the development or maintenance of skin, trophoblasts, and some endothelial cells [12, 58]. GATA3 has been identified as an IHC marker for mammary and urothelial carcinomas in both primary and metastatic setting. It has been suggested useful in the distinction between urothelial versus prostatic adenocarcinoma and metastatic urothelial versus squamous cell carcinoma in the lung . Despite the early promising specificity and sensitivity, however, more recent studies have shown that not all non-urothelial squamous cell carcinomas or prostate cancers to be negative [12, 18, 25–27]. GATA3 can still be of use in the workup of a neoplasm with possible urothelial origin if used with the right context and right combination with other antibodies.
Uroplakins are widely regarded as urothelium-specific proteins of terminal urothelial cell differentiation and have been reported positive in both primary and metastatic urothelial carcinoma [59–62]. Despite being specific to urothelial differentiation, they are not very sensitive as some urothelial carcinomas are not positive for these markers, which limits their practical use and requires the addition of other markers in the workup for a potential urothelial tumor.
Thrombomodulin is a surface glycoprotein involved in the regulation of intravascular coagulation that has been reported to be expressed in a variety of tumors including mesothelioma, endothelial vascular tumors, squamous carcinomas, urothelial carcinoma, and various adenocarcinomas in primary and metastatic setting [63]. The lack of specificity of this marker to urothelial differentiation limits its use in this setting. But as it has been shown in a number of studies mentioned in this section, this marker can be useful when used in combination with other markers in the workup of a potential urothelial tumor.
S100P is a member of the S100 family of proteins that was first discovered in placenta and was thus designated S100P (it is different from the S100 that is widely used in the melanocytic and nerve sheath tumors). Although it was initially identified in the placenta, expression of S100P by IHC has also been described in benign and malignant urothelial cells, pancreatic carcinoma, esophageal squamous mucosa, and breast carcinoma [11] .
Urine-Based Markers for Diagnosis of Bladder Cancer
Fluorescence In Situ Hybridization (UroVysion®, Abbott Molecular, Abbott Park, IL, USA)
UroVysion ® is a FISH probe set with Food and Drug Administration (FDA) approval for use in monitoring tumor recurrence and primary detection of UC in voided urine specimens from patients with gross or microscopic hematuria, but no previous history of UC . The UroVysion® test probe set contains a mixture of four fluorescent labeled DNA probes; a locus-specific probe to the 9p21 band on chromosome 9 and to the centromere of chromosomes 3, 7, and 17. The individual sensitivity of the centromeric probes for chromosome 3, 7, 17 is reported to be 73.7, 76.2, and 61.9 %, respectively, while the sensitivity of homozygous 9p21 deletion for UC has been reported as 28.6 % [64]. The UroVysion® test is based on combination of these probes and the sensitivity and specificity has been reported to be 72 and 83 %, respectively [65]. This test, however, is not free of false positive and false negative results [66]. Inflammation may interfere with proper interpretation of the test .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


