Neurofibroma
Amitabh Srivastava, MD
Key Facts
Terminology
Benign peripheral nerve sheath tumor with heterogeneous admixture of axons, Schwann cells, perineurial cells, and fibroblasts
Most are sporadic; NF1 associated with multiple, large, or plexiform tumors
Clinical Issues
Localized cutaneous NF most common subtype
Diffuse cutaneous NF infiltrate dermis and subcutis
Localized intraneural NF are deep seated and involve larger nerves
Plexiform NF involves multiple nerve fascicles or branches (“bag of worms”)
Massive soft tissue NF involves pelvis, shoulder, or extremities (“localized gigantism”)
Macroscopic Features
Variable size and consistency
Lack degenerative changes seen in schwannomas
Microscopic Pathology
Bundles of spindle cells with angulated or wavy nuclei
Loose, myxoid or thick collagenous matrix
Coarse collagen bundles resemble “shredded carrots”
Residual, central, neurofilament-positive axon fibers present
Atypical NF behave in benign manner
Diagnostic Checklist
Malignant transformation occurs in about 2-10% of plexiform NF
↑ cellularity, atypia, hyperchromasia, mitoses
 Neurofibromas present as fusiform, uninodular or multinodular, well-circumscribed, but unencapsulated tumors. |
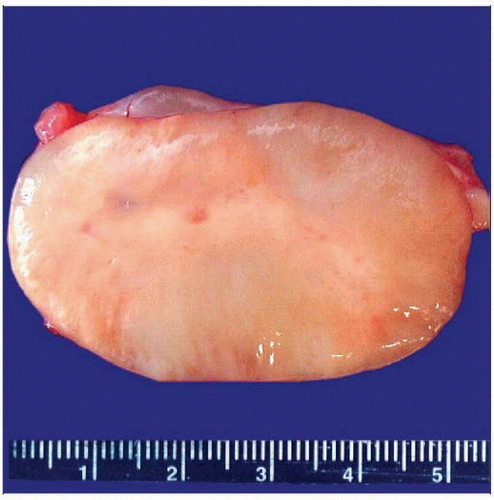 The cut surface of neurofibroma is pale, homogeneous, waxy, and often myxoid in appearance. Degenerative changes typically seen in schwannomas are seldom present in neurofibroma. |
TERMINOLOGY
Abbreviations
Neurofibroma (NF)
Neurofibromatosis type 1 (NF1)
Synonyms
Von Recklinghausen disease = neurofibromatosis type 1
Definitions
Benign peripheral nerve sheath tumor composed of Schwann cells, fibroblasts, perineurial-like cells, and residual nerves in myxoid/collagen matrix
ETIOLOGY/PATHOGENESIS
Histogenesis
Neurofibromas are sporadic in about 90% of cases; others are syndromic in association with NF1
NF1 results from germline mutation in NF1 gene on chromosome 17q11.2
NF1 gene encodes for neurofibromin protein, which is a GTPase-activating protein
Neurofibromin also acts as a tumor suppressor by downregulating Ras and cAMP
Sporadic tumors arise from somatic mutations in NF1
Evidence supporting neoplastic nature of NF
Sporadic tumors are histologically similar to NF1-associated neurofibromas
Tumors are monoclonal on X chromosome inactivation studies
Lesional cells carry NF1 gene deletion
CLINICAL ISSUES
Epidemiology
Incidence
Most common tumor of peripheral nerve
NF1 incidence: 1 in 2,500-4,000 births
Age
Solitary, sporadic lesions: In patients 20-30 years old
Tumors in setting of NF1 present during puberty
Plexiform NF may be congenital
Gender
Affects both sexes equally
Presentation
Most tumors are solitary and sporadic
Superficial cutaneous or localized intraneural NF present as painless, palpable mass
Deep intraneural tumors may present with pain or dysesthesia
Intraspinal (nerve root) NF may show signs of spinal cord compression
Natural History
Slow-growing tumors in most instances
Increased rates of growth may be seen in puberty and pregnancy
Malignant transformation in NF
Rare in sporadic tumors; usually occurs in setting of NF1
Rare in cutaneous NF (0.001%)
More common in plexiform NF (2-10%)
Clinical suspicion for malignant transformation
Rapid enlargement of preexisting NF
Pain or change in neurological symptoms
Treatment
Surgical approaches
Complete resection is curative
Decompression of spinal cord in symptomatic tumors
Prognosis
Recurrence rare, even after partial removal
Subtypes
Localized cutaneous NF
Most common type
Nodular or polypoid, usually well circumscribed
Freely movable, soft, round lesions that elevate skin
Generally not associated with peripheral nerve
Diffuse cutaneous NF
Typically affects children and young adults
Large plaque-like tumors that often affect head and neck region
10% associated with NF1
Diffuse infiltration of dermis and subcutaneous adipose tissue
Entraps dermal vessels, nerves, and adnexa
Spreads along subcutaneous connective tissue septa
Plexiform NF
Usually presents in early childhood
Pathognomonic of NF1 if plexiform architecture is strictly defined
Multinodular lesions involving multiple nerves or nerve branches
“Bag of worms” appearance is characteristic
Generally affects small nerves
Entire extremity may be involved (“elephantiasis neuromatosa”)
Massive soft tissue NF
Tend to be very large, diffuse, or plexiform
Widespread infiltration of adipose tissue and muscle
Result in large pendulous folds of neurofibromatous tissue (“localized gigantism”)
IMAGE FINDINGS
MR Findings
Irregular or bright on T2WI MR
Gadolinium enhancing on T1WI
“Target” sign due to reduced signal in intraneural NF
“Dumbbell” tumors: Intradural and extradural portions of paraspinal tumor acquire shape of dumbbell
MACROSCOPIC FEATURES
General Features
Gray to tan cut surface
Glistening, gelatinous to firm/fibrous consistency
Relatively well circumscribed but not encapsulated
Intraneural NF may be covered by epineurium
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


