Myoepithelioma/Mixed Tumor/Parachordoma
Thomas Mentzel, MD
Key Facts
Terminology
Neoplasms that are composed of epithelial &/or myoepithelial cellular elements in varying proportions
Tumor cells are set in hyalinized to chondromyxoid stroma and may show foci of ductal differentiation
Clinical Issues
Arise usually in adults
Significant number of cases arise in children < 10 years old
Subcutaneous and deep soft tissue
Rare in skin
Upper > lower extremities
Most neoplasms behave in benign fashion
Cytologic atypia represents most reliable prognostic parameter
Treatment: Complete excision
Microscopic Pathology
Characterized by variable morphology
Varying proportions of epithelioid cells, spindled cells, plasmacytoid cells, clear cells
Neoplastic cells are arranged in nests, cords, ductules
Tumor cells are embedded in hyalinized to chondromyxoid stroma
Divergent differentiation (squamous, adipocytic, cartilaginous, osseous) may be present
Nuclear pleomorphism is generally minimal
Few mitoses are usually present (< 2 mitoses per 10 high-power fields)
Dedifferentiation (progression) into frank myoepithelial carcinoma or sarcoma is seen rarely
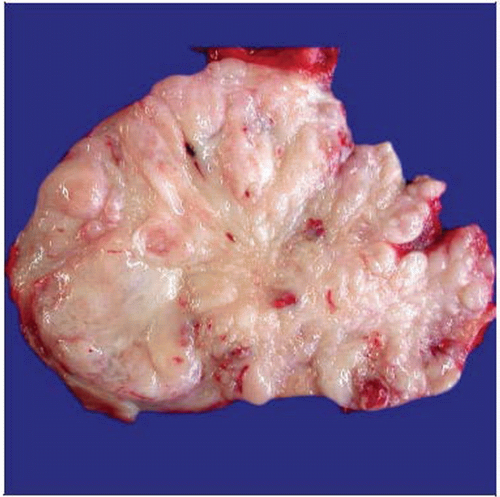 Grossly, this myoepithelioma arising in deep soft tissues represents a rather well-circumscribed, nodular neoplasm with gray-white cut surfaces. |
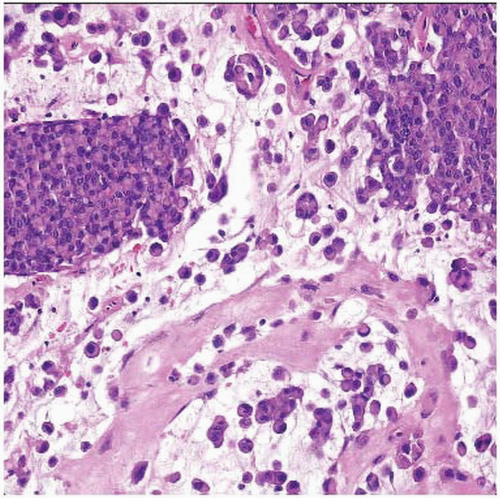 Plasmacytoid myoepithelial tumor cells are arranged in clusters and solid areas and set in a myxohyaline stroma in this example of myoepithelioma of deep soft tissues. |
TERMINOLOGY
Synonyms
Ectomesenchymal chondromyxoid tumor (of tongue)
Definitions
Neoplasms composed of epithelial &/or myoepithelial cellular elements in varying proportions
Tumor cells are set in hyalinized to chondromyxoid stroma and may show foci of ductal differentiation
Show overlap with mixed tumor of skin and soft tissues
Show overlap with myoepithelial carcinoma (malignant myoepithelioma) of skin and soft tissues
CLINICAL ISSUES
Epidemiology
Incidence
Rare neoplasms
Increasingly reported
Age
Arise usually in adults
Significant number of cases arise in children < 10 years old
Gender
Slight male predominance
Site
Subcutaneous and deep soft tissue
Rare in skin
Very rare in bone
Upper > lower extremities > head/neck region > trunk
Less commonly on trunk and in head/neck region
Presentation
Painless mass
Treatment
Surgical approaches
Complete excision
Prognosis
Most neoplasms behave in benign fashion
Minority of cases may recur locally and metastasize
Benign-appearing neoplasms recur in < 20% of cases and do not metastasize
At present, no morphologic features reliably predict prognosis
Cytologic atypia represents most reliable prognostic parameter
Obvious malignant neoplasms behave aggressively
Metastases have been reported in up to 30% of cases
MACROSCOPIC FEATURES
General Features
Usually well-circumscribed neoplasms
MICROSCOPIC PATHOLOGY
Histologic Features
Nodular or lobular growth
Characterized by variable morphology
Varying proportions of epithelioid cells, spindled cells, plasmacytoid cells, clear cells
Cytoplasmic vacuolation is prominent in parachordoma-like cases
Neoplastic cells are arranged in nests, cords, solid formations
Ductal structures are not or only focally present
Tumor cells are embedded in hyalinized to chondromyxoid stroma
Divergent differentiation (squamous, adipocytic, cartilaginous, osseous) may be present
Nuclear pleomorphism is generally minimal
Few mitoses are usually present (< 2 mitoses per 10 high-power fields)
Dedifferentiation (progression) into frank myoepithelial carcinoma or sarcoma is seen rarely
May show loss of INI1 expression in considerable number of cases
Cutaneous myoepithelioma
Rare neoplasms
No ductal differentiation (vs. chondroid syringoma)
Form spectrum with chondroid syringoma and malignant myoepithelioma of skin
No connection with overlying epidermis
May infiltrate into subcutis
Broad variation in regard to growth patterns and cytomorphology
Local recurrences are rare
Lymph node metastases are very rare
Show increased atypia and proliferative activity
Malignant myoepithelioma (myoepithelial carcinoma)
Very rare neoplasms
Tend to be large
Severe cytologic atypia
Pleomorphic tumor cells
Increased proliferative activity
Tumor necrosis
Metastasize in up to 30% of cases (pulmonary and nodal metastases)
Cytologic Features
Epithelioid cells
Round cells, abundant eosinophilic cytoplasm, round vesicular nuclei
Spindled cells
Spindle-shaped tumor cells with fusiform nuclei
Plasmacytoid cells
Abundant eosinophilic cytoplasm, nuclei are located in periphery of cells
Clear cells
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


