, Arthur H. Cohen2, Robert B. Colvin3, J. Charles Jennette4 and Charles E. Alpers5
(1)
Department of Pathology, Microbiology and Immunology, Vanderbilt University Medical Center, Nashville, Tennessee, USA
(2)
Department of Pathology and Laboratory Medicine, Cedars-Sinai Medical Center, Los Angeles, California, USA
(3)
Department of Pathology Harvard Medical School, Massachusetts General Hospital, Boston, Massachusetts, USA
(4)
Department of Pathology and Laboratory Medicine, University of North Carolina, Chapel Hill, North Carolina, USA
(5)
Department of Pathology, University of Washington, Seattle, Washington, USA
Abstract
Patients with plasma cell dyscrasias may have other forms of renal disease than light-chain cast nephropathy. These include the closely related systemic disorders amyloidosis (AL type) and light-chain-deposit disease [1–7]. In the kidneys, although both of these conditions clinically and pathologically affect primarily glomeruli, there is important and often constant involvement of tubular basement membranes, interstitium, and arteries. On rare occasions, the intact monoclonal protein (light and heavy chains) or heavy chain alone may deposit in renal basement membranes and systemically. Consequently, these disorders, originally considered solely of abnormal light-chain pathogenesis and termed by some as light-chain-deposit diseases or nephropathies, are more correctly termed and thought of as monoclonal immunoglobulin deposition diseases [5]. Evaluation of immunoglobulin synthesis by bone marrow cells has determined that incomplete light-chain and/or heavy-chain fragments are produced [8].
Introduction/Clinical Setting
Patients with plasma cell dyscrasias may have other forms of renal disease than light-chain cast nephropathy. These include the closely related systemic disorders amyloidosis (AL type) and light-chain-deposit disease [1–7]. In the kidneys, although both of these conditions clinically and pathologically affect primarily glomeruli, there is important and often constant involvement of tubular basement membranes, interstitium, and arteries. On rare occasions, the intact monoclonal protein (light and heavy chains) or heavy chain alone may deposit in renal basement membranes and systemically. Consequently, these disorders, originally considered solely of abnormal light-chain pathogenesis and termed by some as light-chain-deposit diseases or nephropathies, are more correctly termed and thought of as monoclonal immunoglobulin deposition diseases [5]. Evaluation of immunoglobulin synthesis by bone marrow cells has determined that incomplete light-chain and/or heavy-chain fragments are produced [8].
Light-Chain-Deposition Disease/Heavy-Chain-Deposition Disease
Light-chain-deposit disease is characterized by the nonimmune deposition of a monoclonal light chain in all renal basement membranes as well as the glomerular mesangium. Renal involvement is part of a systemic disease, for virtually all other organs and tissues are also the sites of light-chain deposits. The kidneys are the most important organs involved in terms of clinical manifestations, although some patients can develop significant and fatal cardiac lesions [1–3, 5]. Approximately 80 % of affected patients have an abnormal kappa light chain [9].
Pathologic Findings
Light Microscopy
Light-chain-deposition disease can have many of the light microscopic morphologic features of diabetic nephropathy, especially because of the nodular glomerular lesions and capillary microaneurysms [2, 3, 10, 11].
The light microscopic appearance of glomeruli was initially emphasized as a nodular glomerulopathy with features virtually indistinguishable from nodular diabetic glomerulosclerosis (Fig. 17.1); however, it has become apparent that there is a large spectrum of glomerular morphologies including normal glomeruli, diffuse widening of mesangium, and crescents. The tubular basement membrane deposits often result in the light microscopic appreciation of thickened tubular basement membranes. Careful high-magnification examination of periodic acid-Schiff (PAS)-stained sections may indicate a slightly lighter staining band external to the normal basement membrane [1].
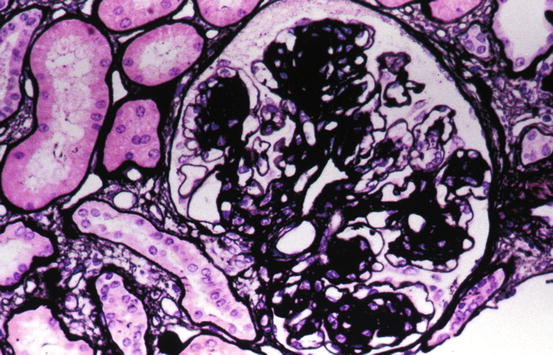
Fig. 17.1
Light-chain-deposition disease with glomerulus with nodular mesangium. This appearance is similar to diabetic nodular glomerulosclerosis (Jones silver stain)
Heavy-chain-deposition disease is characterized by the nonimmunologic binding of an abnormal heavy chain, most commonly immunoglobulin G (IgG), to all basement membranes [8, 11]. The morphologic aspects differ from light-chain-deposit disease in that the glomerular structure is almost always nodular. However, glomerular hypercellularity mimicking membranoproliferative or other proliferative glomerulonephritis may be the dominant morphology [12, 13].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


