Minimally Invasive Sectional and Segmental Hepatic Resection
Kevin T. Nguyen
DEFINITION
The International Hepato-Pancreato-Biliary Association (IHPBA) Brisbane 2000 terminology of liver anatomy and resections1 defines a segmental hepatic resection as a liver resection of one of nine anatomic Couinaud’s segments and a sectional hepatic resection as a liver resection of anatomic sections or sectors (right posterior section [Couinaud’s segments 6 and 7], right anterior section [Couinaud’s segments 5 and 8], left anterior section [Couinaud’s segment 4], or left lateral section [Couinaud’s segments 2 and 3]).
PATIENT HISTORY AND PHYSICAL FINDINGS
The indications for liver resection include primary or metastatic malignant liver lesions or symptomatic benign liver lesions in patients who are surgical candidates. Patients who are candidates for an open liver resection should be considered for a possible minimally invasive approach.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Eovist™-enhanced liver magnetic resonance imaging (MRI) or triphasic, contrast-enhanced computed tomography (CT) scan of the abdomen are virtually equivalent for assessment of disease. They can be complementary in characterizing lesions and determining the probable pathology.
Localize the tumor(s) with respect to the portal structures and hepatic veins to evaluate for resectability. Can an R0 liver resection be performed with curative intent, namely obtaining adequate margins, while leaving a sufficient functional liver remnant with preserved vascular inflow and outflow?
Pay attention to anatomic variants (i.e., replaced/accessory left hepatic artery, replaced/accessory right hepatic artery, trifurcation of the main portal vein, takeoff of the right anterior or right posterior portal vein from the left portal vein, the presence of large inferior hepatic veins, etc.).
SURGICAL MANAGEMENT
Preoperative planning
Where is the transection plane to achieve a negative margin and preserve adequate functional liver reserve?
Where should the port positions be to provide optimal triangulation?
Positioning
Supine with arms abducted. Split-leg positioning is an option preferred by some liver surgeons.
TECHNIQUES
LAPAROSCOPIC LEFT LATERAL SECTIONECTOMY
A purely laparoscopic left lateral sectionectomy can be attempted for hepatic lesions located within segments 2 and/or 3 of the liver (FIG 1).
 FIG 1 • Left lateral sector hepatocellular carcinoma. |
Port Placement
Initial trochar placement: open Hasson approach at a periumbilical position, Veress needle approach in left upper quadrant, or optical separator approach in the left upper quadrant
FIG 2 shows the suggested port positions for a purely laparoscopic left lateral sectionectomy. A 12-mm port at the periumbilical incision, a 12-mm port in left upper quadrant midclavicular line for laparoscopic ultrasound and Endo GIA stapler, a 5-mm port in left upper quadrant midclavicular line, and a 5-mm left subcostal/left flank port.
Mobilization of the Left Lateral Segment
Using a thermal energy device of choice through the right upper quadrant 12-mm port, divide the round ligament at the abdominal wall. The assistant provides countertension through the left-sided 5-mm ports.
Using hook cautery through the right upper quadrant 12-mm port, divide the falciform ligament toward the insertion of hepatic veins into the inferior vena cava (IVC). The assistant provides countertension through the
left-sided 5-mm ports by compressing the liver posteriorly and inferiorly. The avascular adventitia protecting the hepatic veins should be divided to fully expose the anterior aspect of the common trunk of the middle and left hepatic vein.
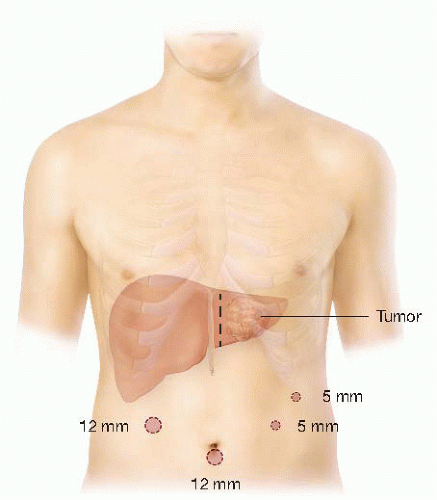
FIG 2 • Port positions for purely laparoscopic left lateral sectionectomy.
Using the hook cautery through the left upper quadrant 5-mm port, divide the left triangular ligament. Optional: Protect the stomach and spleen with a 4 × 4 gauze between the left triangular ligament and stomach.
Using the hook cautery through the left-sided ports, divide the hepatogastric ligament, and identify any replaced or accessory left hepatic artery. The assistant lifts the left lateral section through the right upper quadrant 12-mm port. Clip and ligate any replaced/accessory left hepatic artery.
Rarely, obtaining an adequate margin will dictate extraparenchymal dissection of the portal structures supplying segments 2 and 3. The author’s favored approach is to identify the left hepatic artery near the porta hepatis and dissect it distally to identify and divide the segmental branches of all of the portal structures.
Parenchymal Transection of the Liver
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


