Appendectomy: Laparoscopic Technique
Roosevelt Fajardo
DEFINITION
Acute appendicitis is the most frequent cause of acute surgical abdominal pain seen in the emergency services around the world. Close to 7% of the total world population will suffer from appendicitis at some point in their lives. Although it may occur at any age, its incidence is higher in childhood, with a peak incidence between 10 and 30 years of age. It is more frequent in men, with a male-to-female ratio of 1.4:1. Advances in laparoscopic surgery around the world have made laparoscopic appendectomy a safe and simple procedure.
DIFFERENTIAL DIAGNOSIS
Urinary tract infection
Intestinal obstruction
Acute cholecystitis
Mesenteric adenitis
Meckel’s diverticulitis
Colonic diverticulitis
Right ureteric colic
Ectopic pregnancy
Salpingitis, pelvic inflammatory disease
Ruptured ovarian follicle
Gastroenteritis
Terminal ileitis
PATIENT HISTORY AND PHYSICAL FINDINGS
Despite advances in diagnostic imaging, diagnosis of acute appendicitis continues to be predominantly clinical. A good clinical history and a thorough physical examination should provide the surgeon with a high degree of suspicion. The characteristic clinical picture is one of abdominal pain that exacerbates with movement, starting in the periumbilical region and then migrating to the right lower quadrant. Fever, anorexia, nausea, and vomiting are frequent.
The Alvarado score, a clinical scoring system used in the diagnosis of appendicitis, assigns points to six clinical items and two laboratory measurements with a maximum possible total of 10 points. With scores greater than 5, the probability of acute appendicitis increases.
A popular mnemonic used to remember the Alvarado score factors is MANTRELS: Migration to the right iliac fossa, Anorexia, Nausea/Vomiting, Tenderness in the right iliac fossa, Rebound pain, Elevated temperature (fever), Leukocytosis, and Shift of leukocytes to the left. Due to the popularity of this mnemonic, the Alvarado score is sometimes referred to as the MANTRELS score.
The location of the appendix may change the clinical presentation. With the appendix in a retrocecal location, patients may present with right flank pain. With an appendix in a pelvic location, patients typically present with urinary symptoms and diarrhea.
IMAGING AND OTHER DIAGNOSTIC STUDIES
The hemogram typically shows a leukocytosis, with a leftsided shift. Female patients in fertile age should have a pregnancy test prior to surgery.
Ultrasound (FIG 1) has shown to have 86% sensitivity and 81% specificity for the diagnosis of acute appendicitis and has the benefit of not being invasive, but it is operator dependent.
Computerized axial tomography (CAT; FIG 2) scan, with a 94% sensitivity and a 95% specificity, has been shown to be the most accurate imaging study for the diagnosis of acute appendicitis but is expensive and may delay surgical intervention.
Magnetic resonance imaging (MRI) is reserved for patients who cannot be exposed to radiation, such as pregnant women suspected of having appendicitis.
SURGICAL MANAGEMENT
Indications
Same indications than for open appendectomy
Any patient with diagnosis of appendicitis who can tolerate pneumoperitoneum and general anesthesia, provided that trained staff and the necessary equipment for a safe procedure are available
Preoperative Planning
Appropriate prophylactic antibiotic should be administered 30 minutes before surgery.
Decompression of the bladder by voiding before surgery or by using a Foley catheter may avoid injury of the bladder during trocar placement.
Patient and Team Positioning
The patient is secured to the table with the arms padded and tucked to the side.
The surgeon and the camera operator stand on the patient’s left side (FIG 3).
The monitor is placed in front of the surgeon (at eye level) on the patient’s right side.
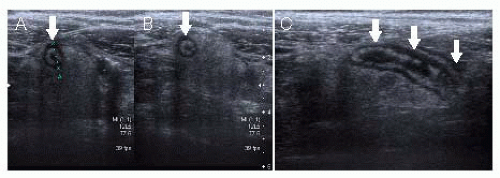 FIG 1 • Ultrasound imaging in appendicitis. Arrows show a distended appendix with a thickened wall. A and B show transverse views of the appendix. C shows a longitudinal view of the appendix. |
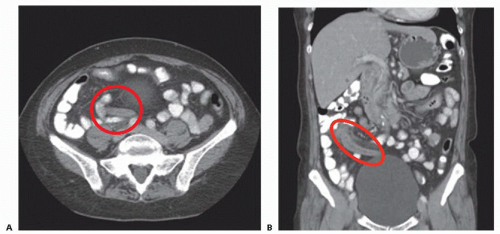 FIG 2 • CAT scan imaging in appendicitis. A: Axial view. B: Coronal view. Red circles show acute appendicitis with periappendiceal inflammation. |
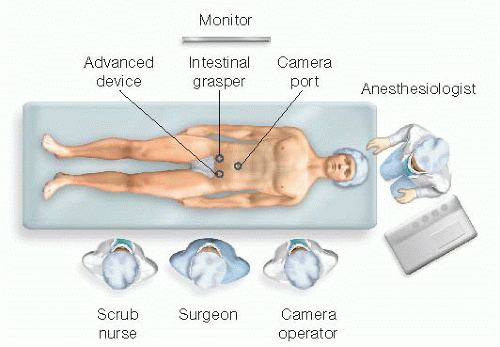 FIG 3 • Patient, port, team, and operating room setup. |
Port Placement
A traditional laparoscopic appendectomy is performed using a three-port system (FIGS 3 and 4). The surgeon should be able to work two-handed.
The ports are triangulated to enhance maneuverability and exposure.
A 10-mm Hasson trocar is inserted in the umbilicus. This trocar will be used for CO2 insufflation and also as a camera port.
A 12-mm trocar is inserted in the left lower quadrant. In addition to being the main dissection port, this port will be used for the stapler and also as an extraction site. If a good quality 5-mm camera is available, then a 5-mm port can be inserted in this location; in this alternative setup, the specimen would be retrieved through the umbilical port site.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


