Patient Story
A 40-year-old woman with diabetes comes to the clinic with blood sugar in the 400s because she ran out of insulin a few weeks ago. She appears poorly groomed and has nicotine stains on her fingertips. Excoriated lesions (Figure 238-1) are noted on her forearms and face. She reports no itching at this moment, but when asked confirms that she regularly smokes methamphetamine. The diagnosis of her skin condition is meth mites. She acknowledges that she picks at her skin when she is high on meth. The physician asks her if she wants help to get off the meth so she can care for her health and well-being. She breaks down in tears and says that her craving for meth is very strong, but she is willing to try something because she knows the meth is ruining her body and life.

Introduction
Epidemiology
- Worldwide, compared to other drugs of abuse, only marijuana is used more often than amphetamine/methamphetamine.1
- The lifetime prevalence (“ever-used”) rate for methamphetamine was 2.1% for 12th graders in the 2011 Monitoring the Future study, which surveys 50,000 students in 8th, 10th, and 12th grades in 420 schools nationwide annually. This has decreased from 1999, when the lifetime prevalence for methamphetamine use in 12th graders was 8.2%. For comparison, marijuana/hashish had a lifetime prevalence in 12th graders of 45.5% and 49.7% in 2011 and 1999, respectively.2
- Stimulants (methamphetamine and amphetamine) accounted for 9.6% of nationwide emergency department visits involving use of illicit drugs in 2009, with the highest incidence in those from 18 to 44 years old.3
- Methamphetamine use is associated with white or Native American race; residence in the west or south; having an ever-incarcerated father; marijuana, cocaine, intravenous drug use; and men who have sex with men (MSM).4
- Analysis of methamphetamine found in workforce drug testing done nationwide in 2010 by Quest Diagnostics showed the highest rates of use in western and midwestern states, with relative sparing of eastern states. Highest prevalence (more than twice the national average) was found in Hawaii, Arkansas, Oklahoma, Nevada, California, Wyoming, Utah, and Arizona.5
- Methamphetamine is a Schedule II stimulant with legitimate medical uses, including the treatment of narcolepsy and attention deficit hyperactivity disorder.
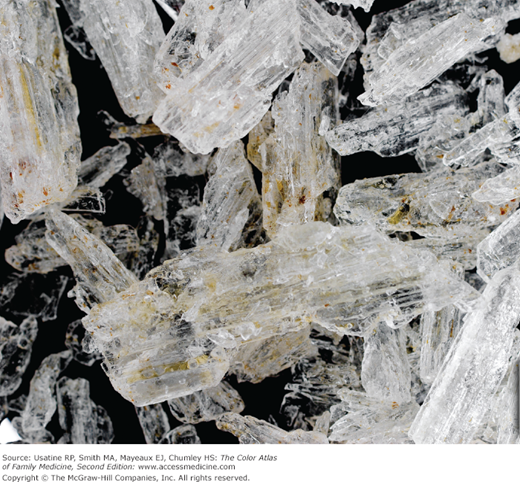
- Methamphetamine is known on the street as meth, crank, ice (Figure 238-2), and crystal. It is abused by smoking, injecting, snorting, or oral ingestion. Smoking or injecting the drug gives an intense, short-lived “flash” or rush. Snorting or oral ingestion creates euphoria but no rush.
- Methamphetamine can be manufactured from inexpensive, readily available chemicals using recipes easily found on the Internet and in books (Figure 238-3).
- Common household and industrial chemicals used to make methamphetamine include pseudoephedrine and ephedrine (cold tablets), red phosphorus (matches/road flares), iodine (teat dip or flakes/crystal), methanol (gasoline additives), muriatic acid (used in swimming pools), anhydrous ammonia (farm fertilizer), sodium hydroxide (lye), sulfuric acid (drain cleaner), toluene (brake cleaner), and ether (engine starter).7
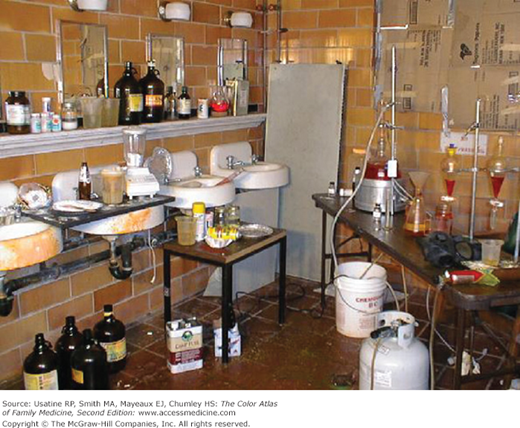
- The “meth laboratory,” the site of small-scale methamphetamine production (Figure 238-4), brings with it many hazards, including exposure to toxic chemicals for the meth cooks themselves, their children, and law enforcement, medical, and fire personnel entering the laboratory in the course of their duties. Explosions and fires at meth laboratories are common. Improper disposal of the toxic chemicals used in the laboratories frequently leads to environmental contamination.8
- Effects of methamphetamine, such as euphoria, increased libido, and impaired judgment, may lead to increased high-risk sexual behaviors, such as unprotected sexual intercourse and contact with multiple sexual partners. As a result, methamphetamine users are at increased risk of contracting sexually transmitted infections, including HIV.
Etiology and Pathophysiology
- Methamphetamine acts as a central nervous system stimulant by blocking presynaptic reuptake of dopamine, norepinephrine, and serotonin.
- Compared to amphetamines, methamphetamine has an increased ability to cross the blood-brain barrier and has a prolonged half-life (10 to 12 hours). This leads to faster-onset, more intense, and longer-lasting effects when compared to amphetamine.
- Intended effects of methamphetamine use include euphoria, increased energy, a heightened sense of alertness, and increased libido.
- Unintended effects include increased heart rate, blood pressure, and body temperature; headaches; nausea; anxiety; aggression; paranoia; visual and auditory hallucinations; insomnia; tremors; and cardiac arrhythmias.
- With chronic abuse, neurologic manifestations include confusion, poor concentration, depression, paranoia, and psychosis. Weight loss and dental decay can occur. The face and body become atrophic and gaunt, making the chronic methamphetamine user appear older than their stated age.
- Methamphetamine users may experience formication, the hallucination that bugs are crawling under the skin. The skin excoriations resulting from picking at the imagined bugs are known as “meth mites” (Figures 238-1, 238-5, and 238-6).
- The rampant dental caries and gingivitis commonly seen in methamphetamine users is known as “meth mouth” (Figures 238-7 and 238-8). The causes of meth mouth are multiple. Vasoconstriction leads to decreased saliva production and dry mouth, which often result in consumption of large amounts of sugar-containing beverages. Methamphetamine users often neglect their oral hygiene when preoccupied with obtaining and using the drug. Methamphetamine-induced bruxism also damages the teeth. Neglect of early symptoms and lack of access to or failure to seek dental care often lead to unsalvageable teeth that can only be extracted.9–11




