Prescribing chemotherapy medications (checkpoint 1). Health care providers who prescribe, prepare, and administer chemotherapy drugs should be familiar with the entire treatment regimen. A prescriber should order all the medications necessary for the entire treatment regimen, including hydration and supportive care orders, at the same time and prior to administration of any of the medications. When prescribing chemotherapy regimens based on a patient’s weight (or BSA, which relies on weight), weight data and trends in patient weight should be evaluated to be sure the correct information is used. In CPOE, order sets may assist in completing all relevant orders of a treatment regimen at the same time. Requiring all treatment details in advance ensures that orders can be checked for completeness and accuracy and compliance with planned treatment.
Institutions should establish policies regarding whether chemotherapy may be prescribed by physicians-in-training (e.g., medical fellows) and nonphysician health care providers with prescribing privileges (e.g., nurse practitioners, physician assistants). If the institution allows prescriptions by these individuals, these orders should be verified by at least one medically responsible person, other than the prescriber, who is knowledgeable about medical oncology.
When orders for chemotherapy drugs must be countersigned by a second medically responsible individual, the person who countersigns the medication orders should critically evaluate each order for a chemotherapy treatment. This is checkpoint 1. The orders should be compared with patient-specific data and verified against original reference sources that describe the treatment regimen (e.g., a published article, validated standard reference text, investigational protocol). If the patient is taking part in an investigational study, verification of enrollment onto the trial and of informed consent should be reviewed.
Preparing chemotherapy medications (checkpoints 2–4). Checkpoint 2 requires persons receiving a prescriber’s order for chemotherapy medications to review the original medication orders and independently verify them against published standards (e.g., product package labeling, reports published in professional journals, treatment protocols, standard reference textbooks) and determine appropriateness based on patient-specific information. The dose per container and the total course dose should be verified at this checkpoint.
Because erroneous information sometimes appears in published information, orders for non-investigational chemotherapy medications should be verified against the primary reference in which the specific treatment was described (e.g., published reports, study protocols, meeting proceedings). If a primary reference is not available, the treatment regimen should be confirmed with a resource that previously had been validated as accurately describing the planned treatment (locally compiled handbooks, guides, and compendia) or at least two alternative publications, including reviews and reference textbooks.11,34 Investigational drug doses and administration schedules must be verified against a study protocol that was approved by all relevant regulatory agencies and study sponsors (e.g., institutional review board, National Cancer Institute, FDA). Protocol amendments should be distributed immediately and be readily available for reference. In addition, order templates should be updated as soon as possible, especially for drug dose or preparation changes.
Although preprinted order forms and CPOE preclude the necessity of repeatedly verifying drug names, dosages, routes, and schedules, all medication orders should be evaluated for completeness, compliance with the planned regimen, and, during repeated courses, deviations from previous treatments by following these recommendations:
- The date a patient was last treated and the next planned treatment date should be compared to ensure that an appropriate interval has elapsed since treatment was last administered.
- Measurements from which a patient’s medication dosage and administration rate are calculated should be confirmed (e.g., height, weight, BSA). Institutions should develop policies and procedures regarding when patient-specific data (e.g., height, weight, BSA) should be re-measured. It is important to review trends in height and weight as a double check to ensure there were no errors in documentation.
- Appropriate laboratory test and physical assessment values should be evaluated and primary treatment references should be consulted to determine whether they are within acceptable ranges or if treatment modifications are indicated.
- A patient’s allergy, drug sensitivity, and adverse drug effect histories and his or her current medication profile should be evaluated for potential drug interactions with planned chemotherapy treatment.
For patients who receive treatment in clinical trials in which more than one primary or ancillary treatments are prescribed (e.g., dose- and duration-escalating studies), treatment assignment and dosage and administration schedule modifications should be confirmed with at least one person directly associated with the clinical trial, other than the prescriber (e.g., the principal investigator, an associate investigator, research nurses or pharmacists, a study coordinator or chairperson). The prescriber should be consulted when expected treatment modifications were not ordered or when nonstandard modifications were prescribed.
Instructions for diluents, drug administration sequence and duration, number of doses, and starting date and time should be checked. To ensure that appropriate ancillary and supportive medications that facilitate chemotherapy drug delivery and those required by protocol have been prescribed and are complete and accurate (e.g., premedications, hydration, cytoprotectant and “rescue” medications, antiemetics, hematopoietic growth factors), their orders should be reviewed and confirmed. Discrepancies between prescribed medications and planned treatment should be brought to the prescriber’s attention and resolved before medication preparation proceeds.
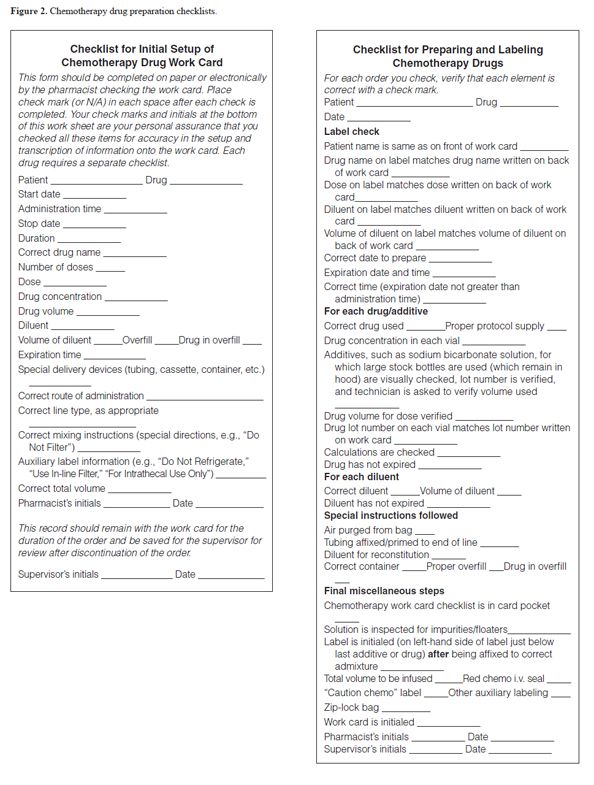
At checkpoint 3, after treatment orders have been verified, all work related to medication-order processing and preparation accuracy should be routinely documented in a standardized format, either on paper or electronically. Drug preparation work sheets (sometimes referred to as work cards or admixture or compounding logs, sheets, and cards) identify the drug products prepared for each patient and the persons who prepared and checked the medications. Although layout and design may vary among work sheets, and data may be organized as a continuous log in which each drug product appears on separate, consecutive lines or as a separate record for each patient, all work sheets should detail the techniques used in preparing the drug products. They should also identify special preparation and dispensing information, such as the indication of special product containers, requirements for filtration, the need for special diluents, intermediate dilution steps, and how and when administration sets should be attached to the drug product container. Order processing, drug preparation, and processing records should be confirmed by a second individual (preferably a pharmacist).11,12 The calculations written on preparation work sheets should be independently verified by a second health care provider who did not prepare the work sheet. Independent verification should include checking the work sheet for completeness and accuracy of content, with particular attention given to special preparation instructions. A checklist, whether paper or electronic, that identifies the necessary elements in chemotherapy drug preparation may be a helpful reference (Figure 2).11 Technology can serve as a surrogate checklist, if practitioners follow procedures in using appropriately developed and applied software.
At checkpoint 4, drug products should be checked, after preparation, against both the preparation work sheet and the original order by an individual who was not involved in preparing the work sheet. Checklists may also be helpful for this step.11
Dispensing chemotherapy medications (checkpoint 5). Checkpoint 5 requires persons dispensing medications to patients or caregivers for outpatient use to verify a patient’s identity when a medication is dispensed. Patients who self-administer their medications or personal caregivers should visually examine the medication, confirm whether its appearance meets their expectations, and compare its instructions with information they received from their health care providers (e.g., a chemotherapy calendar).
Dispensing and administering chemotherapy medications (checkpoints 6–9). At checkpoint 6, before starting treatment, each chemotherapy medication should be checked independently against the prescriber’s orders by at least two individuals who are trained and competent to administer chemotherapy medications. All dosage- and administration-rate-related calculations should be independently verified. This includes any infusion pump rate settings, which should be checked at the initiation of each container of the infusion, periodically throughout the infusion, and whenever a new nurse assumes care for the patient. Health care providers should routinely confirm that the medication will be administered to the intended patient by comparing a patient’s name and unique identifying code or number with medication labels (e.g., alpha–numeric characters or bar codes) and that a drug product’s identity, ancillary components (e.g., additional medications, diluent, and vehicle solutions), route of administration, and schedule are correct.
At checkpoint 7, health care providers should examine the medication container and note whether the content’s general appearance is what was expected. Many parenteral chemotherapy products have distinctive colors, and product coloration should be confirmed before administration.
At checkpoint 8, patients who self-administer their medications (or receive it from personal caregivers) should carefully read the container’s label to confirm the product’s identity and review its instructions for use (schedule of dosing, whether to take with or without food) each time they take a medication.
At checkpoint 9, patients should be encouraged to ask questions about their treatment before its administration and compare its appearance and medication label with information they received about the treatment. Patient identification using two identifiers should occur prior to chemotherapy administration. Whenever possible, barcode-driven administration should be used.40
In ambulatory care practice, it is common for patients to receive parenteral chemotherapy medications in a setting where a physician and a nurse (or other health care professional) complete all tasks related to prescribing, preparing, administering, and monitoring treatment without a pharmacist’s participation. Under these circumstances, the health care providers involved should perform independent double checks and be involved in the entire process. The person preparing chemotherapy medications should work from written orders.
Monitoring (checkpoint 10). Chemotherapy agents are usually expected to produce adverse events, so it is sometimes difficult to detect possible medication errors resulting from failure at one of the prior checkpoints. However, a vigilant health care team might discover a potential error sooner if they are knowledgeable about the expected adverse effects and are vigilant for either exaggerated or unexpected adverse effects.
For all chemotherapy agents administered at a health care institution, the patient’s clinical status should be assessed on each day of chemotherapy administration. Vital signs should be taken and a standardized assessment for possible toxicities should be performed.
For oral chemotherapy agents, assurance that patients understand how to take their chemotherapy medicine should be assessed initially and then at each patient encounter. An assessment for adherence should be performed at each clinic visit. Patients should be taught how to recognize and report expected and unexpected toxicities.
Recommendations for Prescribing Systems and Prescribers
Chemotherapy prescribing is complicated by numerous medical publications that report indications, dosages, and administration schedules inconsistent with FDA-approved product labeling. Chemotherapy treatments frequently involve off-label uses based on preliminary reports, promising information from abstracts, and compendia information. Prescribers must exercise great care in correctly interpreting this information and clearly communicating orders for chemotherapy medications with other health care providers.
Health-system administrators should require orders for all chemotherapy medications and other high-risk drugs prescribed by physicians-in-training or non-physician prescribers to be countersigned by a senior physician with expertise in the specialty to safeguard against errors in interpretation and prescribing. Health care providers seeking privileges for prescribing chemotherapy drugs should complete an orientation to local policies and procedures related to prescribing chemotherapy before they are permitted to order them for patient care.
Health care providers should locally develop standardized dosage and administration schedule modifications for each chemotherapy medication. Treatment modifications may be appropriate for patients with the following characteristics: (1) preexisting pathologies that predispose a patient to adverse effects from treatment with particular chemotherapies (e.g., withholding or decreasing bleomycin dosages in patients with preexisting pulmonary dysfunction or cardiotoxic agents in patients with congestive heart failure); (2) a history of severe, prolonged, or cumulative adverse effects after previous chemotherapy treatments; (3) impaired physiological function that predisposes patients to altered pharmacodynamic responses (e.g., renal or hepatic impairment); (4) low or decreased performance status; and (5) patients on multiple medications with a potential for a drug interaction with a particular chemotherapy.
Health care providers should also establish for their institutions standardized guidelines for prescribing drugs that are routinely administered concomitantly with chemotherapy medications. Medication-use guidelines for supportive care and ancillary agents (e.g., antiemetics, hydration, chemoprotectants) should be made accessible to all health care providers who prescribe, prepare, and administer chemotherapy drugs and for persons who perform clinical monitoring.
When generating medication orders in a setting where preprinted ordering forms, CPOE, and other electronic and mechanical means (e.g., e-prescribing) are not available, prescribers should legibly print the names of medications, dosages, routes of administration, and administration schedules in plain block letters and Arabic numerals. Medication orders should include the indications for which they are prescribed (e.g., for sore mouth, for nausea, for chronic lymphocytic leukemia).
When chemotherapy treatment (ordering, preparing, and administering) is coordinated at a single location, it is the prescriber’s responsibility (or in the conduct of clinical trials, it is the principal investigator’s responsibility) to provide information about the treatment (e.g., protocols, publication reprints) to those who prepare and administer medications and monitor patient outcomes. It remains the prescriber’s responsibility to answer questions and provide information to other health care providers when treatment is implemented in a place that is geographically separate from the prescriber’s location. Prescribers, clinical investigators, and medically responsible staff should provide to health care providers who prepare and administer chemotherapy medications a complete printed (or electronically reproduced) copy of the treatment regimen.
General Guidelines for Prescribing Chemotherapy Medications.11,13,20,41 The following are general guidelines for prescribing chemotherapy drugs:
- Instructions for medication regimens should be explicit, complete, clear, and easy to follow. Treatment regimens should be described accurately and consistently in all written, published, or circulated materials in which chemotherapy medication use is described.
- The patient’s medical record should contain a justification for the chemotherapy treatment plan (e.g., FDA product labeling, a primary literature reference, institutionally approved guidelines, national consensus guidelines, or an investigational protocol).
- Medication-use systems should require health care providers to use standardized vocabulary and nomenclature for describing treatment with chemotherapy medications. “Tallman” lettering should be used for written and electronic orders.
- Prescribers should use uniform and consistent notations to express quantifiable amounts (dosage, concentration, volume, and time).
- Prescribers should never trail a whole number with a decimal point followed by a zero (e.g., write “5 mg,” not “5.0 mg”).
- When writing amounts less than one, the expression should be written with a leading zero preceding the decimal point (e.g., “0.125 mg”).
- All treatment plans and medication orders should identify the dosage (as a function of body weight, BSA, or other dosing factors) and the calculated dose. Total course dose should be included in circumstances in which a single infusion container is designed to provide multiple days of treatment (e.g. 7-day cladridine infusion).
- When treatment day enumeration is arbitrary, day 1 typically describes the day treatment commences. In contrast, hematopoietic progenitor-cell transplantation regimens often include day 0, and significant treatment-related events before and after a progenitor-cell graft is administered are distinguished by negative (minus) and positive (plus) prefixes, respectively.
- All medications that are a part of the treatment regimen (e.g., oral chemotherapies) should be included, indicating where the product will be filled or dispensed.
- Recommendations for proper medication storage should also be included. Cancer patients must often travel long distances to receive care, so guidance and support (provision of coolers and ice packets for refrigerated medications) to properly store medications when in transit as well as at home.
In some cases, CPOE can be used to promote best practices (e.g., eliminating the use of trailing and leading zeros [items 4 and 5 above]).
Specific Recommendations for Parenterally Administered Medications.20 Health care providers should adhere to the following guidelines for parenteral chemotherapy drugs:
- In treatment plans and orders, doses should be expressed as the total amount of medication to be administered from a single container (i.e., the total amount of medication per syringe, bag, or other container).
- For medication admixtures that can be prepared in more than one way, practitioners should institute a priori, standard, and consistent methods directing how each medication will be prepared and administered.
- When a medication with extended stability is administered from a single container for more than 24 hours, a prescriber’s order for treatment should specify the amount of medication to be administered during each 24-hour interval.20 For example, a medication order for a patient with a BSA of 2 m2 should read: Drug XYZ (8 mg/m2/day × 3 days) 48 mg in 150 mL 0.9% sodium chloride injection by continuous intravenous infusion over 72 hours. Start on 04/01/2001 at 0800 (total dose/cycle = 48 mg).
Specific Recommendations for Orally Administered Chemo-therapy Medications.20,42 Prescribing orally administered chemotherapy agents presents unique challenges for health care providers due to the greater responsibility placed upon patients to manage their own care and patients’ perception that these agents may be less dangerous than parentally administered agents. Health care providers should adhere to the following recommendations when oral medications are the prescribed chemotherapy treatment or when oral chemotherapy is included as part of the treatment regimen:
1. In treatment plans and medication orders, drug doses and schedules should be described as the amount of medication to be taken per dose, not as a total daily dose that is to be taken in divided doses.
2. In treatment plans, medication orders, and instructions to a patient, the number of doses to be administered or taken should be clearly identified.
3. Doses for solid orally administered dosage forms should specify whether and how doses are to be rounded to the nearest capsule or tablet strength. If the calculated dose can’t be provided based on the available dosage forms, the following alternatives can be considered:
a. whether tablet formulations should be broken (if not a hazardous drug);
b. whether an alternative dosage method or formulation is appropriate; or
c. whether alternate day dosing is appropriate based on the pharmacokinetic and pharmacodynamic properties of the medication. The goal of alternate day dosing is to fulfill the total weekly dose rather than giving the exact daily dose (e.g., if an agent is to be given 175 mg daily for 2 weeks, but the drug is only available in 50 mg capsules, consider alternate day dosing by giving 200 mg on one day and 150 mg on the next day). If alternate day dosing is used, then instructions that say “take X tablets on odd days and X tablets on even days” should be avoided, as two consecutive odd days may occur when transitioning from one month to another. For example: January 31 and February 1.
4. Only the quantity needed to cover the administration period until the next clinical evaluation should be ordered.
5. If appropriate, instructions should address how medications are to be taken with respect to food ingestion and indicate whether particular types of food may affect medication activity.
6. Oral chemotherapy medication orders should be included with parenteral chemotherapy orders to allow for appropriate screening and safety checks.
7. Oral chemotherapy medication orders should be included on the patient’s home medication list to allow for appropriate screening and safety checks.
8. Oral chemotherapy medication orders should be communicated to the pharmacist for appropriate screening and safety checks.
9. Patient instructions should address what to do if a dose is missed.
10. Patients should be provided with explicit instructions regarding what adverse effects to expect, which ones require a telephone call to a provider, and who and where to call.
11. Instructions should describe safe handling, storage, and disposal of oral chemotherapy.
12. Essential ancillary medications and supportive care that accompany a chemotherapy treatment regimen should be explicitly identified.
13. Refills on oral chemotherapy medications should be discouraged, when feasible.
14. Patients should be appropriately educated regarding access and cost issues (e.g., regarding specialty pharmacies, prior authorization, out-of-pocket costs, and options for pharmaceutical manufacturer or copay assistance).
Recommendations for Medication Preparation and Dispensing Systems and Roles for Pharmacists
For each practice setting, persons representing the various health care disciplines that prescribe, prepare, and administer chemotherapy medications should participate in planning and managing local medication-use systems.
Standardized Medication Preparation Guidelines. Health care providers should establish standardized guidelines for reconstituting, diluting, admixing, packaging, and labeling commonly used chemotherapy and other medications that are routinely administered with chemotherapy. Each practice facility should also establish a standardized method for labeling multidose vials and reconstituted drug products. Standardized medication preparation guidelines should be prominently displayed (e.g., as a chart) for easy accessibility in areas where orders are processed and medications prepared. Policies should be developed for prescribing of oral chemotherapy that are not being dispensed by the health system. Instructions for patient counseling, safe handling, and disposal should be included in these policies.
Policies and procedures should be developed for situations in which medications are prepared at facilities that are geographically removed from where treatment is administered. Procedural protocols should describe requirements for medication packaging, storage conditions during transportation, duration of transport, and handling after delivery. Medication couriers should receive training in organizational policies for handling medications and should immediately report when conditions and handling practices deviate from procedural standards. In addition, handling procedures should ensure patient confidentiality and provide guidelines for emergency situations, such as hazardous-drug spills.
Persons who prepare and dispense chemotherapy medications should ensure timely drug delivery to patients and patient-care areas after receiving written orders. If dispensing is delayed for any reason, health care providers awaiting the medications should be notified.11
Quality Assurance and Improvement. In collaboration with health care providers who prescribe and administer medications, pharmacists and persons who prepare and dispense chemotherapy should take the initiative in developing and managing quality-assurance and quality improvement programs for their medication-use systems. These programs should include surveillance and reporting systems, FMEAs, and root-cause analysis, when appropriate, that track potential and actual medication errors, evaluate the proximal causes of errors among processes and systems, and identify preventive measures.11,43 The major advantage of multidisciplinary participation is that each discipline’s perspectives and methods for conceptualizing system flaws and solutions can be incorporated in designing strategies for preventing medication errors. Confidential reporting is essential to the success of a medication-error surveillance and reporting system. Only by understanding what causes and contributes to errors can the number of errors be reduced. In designing a medication-error surveillance and reporting system, strategic emphasis should be placed on understanding why errors occur and not on blaming or censuring personnel.44 Further, proactive assessment of the chemotherapy-use process should be conducted.
Orientation on Medication-Error Reduction. Pharmacy supervisors and managers should develop an orientation program about medication errors commonly associated with chemotherapy medications for training of pharmacy personnel who prepare and dispense chemotherapy. Pharmacists should develop ongoing interprofessional educational programs that focus awareness on potential medication errors with chemotherapy medications, strategies for preventing errors, and local and national medication-error reporting and evaluation systems for all practitioners who have direct patient contact.
Pharmacists should engage the support of medical and nursing administrators and supervisors to encourage their staff (particularly those in professional training programs) to complete chemotherapy medication-error awareness programs.30 Educational programs should be discipline specific. Program content should include medication-error case scenarios, problem-solving to prevent and mitigate medication errors, and discussion about the effects that medication errors have on patients’ quality of life and the health system.11,31
Standardized Drug Procurement and Storage. Pharmacists who select and procure drugs should strive to minimize or eliminate look-alike drug product containers and limit the availability of different vial sizes for parenteral medications whenever possible.12 Frequent additions to the variety of available drug products and changes among alternative manufacturers’ drug products can contribute to medication-use errors and should be avoided. If it is necessary to change manufacturers, health care organizations should develop a process to ensure staff are educated about the new product and that computer systems have the appropriate manufacturer’s information. When practical, drug products with similar names and packaging should not be stored next to each other. Medication-use systems that involve a formulary should separate nonformulary products from those that are on the formulary. Health care providers should familiarize themselves with chemotherapy drugs that are not on formulary before prescribing, preparing, and administering them.
Standardized Medication Preparation and Dispensing. Chemotherapy medications should be dispensed in ready-to-administer dosage forms whenever possible. Generally, chemotherapy for intermittent parenteral administration should be prepared so that each medication container has only one dose. The risk of incorrect medication use is increased when the amount of drug dispensed in a single container exceeds the amount to be administered during a 24-hour period. It is essential that individuals and committees responsible for developing and overseeing medication-use systems establish guidelines on whether prescribers may order chemotherapy preparations to be administered from a single container for more than 24 hours. In all practices where parenteral drugs with extended stability (more than 24 hours) are sanctioned, it is imperative that the duration of their use is clearly labeled and that health care providers are trained to correctly prescribe, prepare, and administer them.20
When preparing a chemotherapy admixture, a quantity of medication that most closely approximates the prescribed dose should be segregated from other drug supplies. For treatment regimens that include two or more drugs, especially when medications are to be administered by different routes, the medications should be physically segregated during preparation and when administered. Compounded medications should be prepared one at a time, using standardized techniques whenever possible.
The chemotherapy preparation process should include an independent double check by two separate individuals of the correct drug, diluents, administration containers, and volume measurements before the solutions are transferred to the final administration container. A person other than the individual who selected the components of the preparation (drug and diluent) and measured the volume of diluent solutions used to reconstitute the medications should visually confirm the correct product(s) and measurement(s) before the solutions are transferred from the measuring device to the drug vial for reconstituted drugs and to the final administration container. Post hoc or proxy methods for checking medication preparation, including pulling back syringe plungers to demonstrate the volume of fluid that was injected into the secondary container, should not be used as the sole method for verifying chemotherapy product preparation. Verification may be accomplished by direct visual inspection; remote monitoring through telepharmacy applications (with pictures); or by weighing syringes, other transfer devices, and intermediate product containers before fluid transfer is completed. Whenever possible, methods that allow direct observation of product preparation should be used. The actual original medication vials and diluents that were used during preparation must be present for inspection during the verification process.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


