Chapter 16 Male Genitalia, Hernias, and Rectal Exam
“God gave Man the penis and the brain as His two greatest gifts.
Unfortunately, He made it so that Man could only use one at a time.”
A. Male Genitalia
1 What are the main components of the male reproductive system?
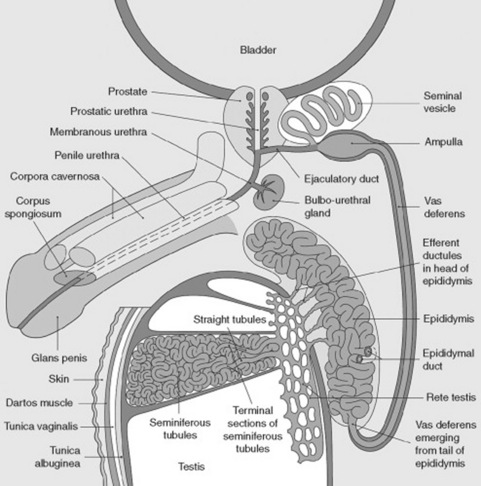
The penis, the scrotum (with testicle, epididymis, and deferens), the seminal vesicles, and the prostate (Fig. 16-1).


(1) Penis
4 Describe the anatomy of the penis.
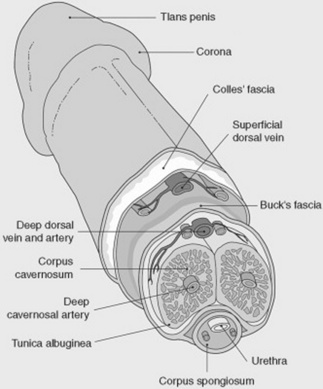
The penis consists of a shaft, formed by three juxtaposed columns of spongy and vascular tissue: the corpora cavernosa. These can be temporarily filled with blood, thus providing a unique erectile capacity to the organ. The distal tip of the penis consists of a cone-shaped structure called the glans (“acorn” in Latin), which contains the vertical slit-like opening of the urethra (urethral meatus). The glans is separated from the shaft by a circular sulcus called the corona (“crown” in Latin), which in uncircumcised men is covered in a hood-like fashion by the prepuce or foreskin, a fold surgically removed during circumcision. All areas must be examined (see Fig. 16-2).
5 What steps should I take to properly examine the penis?
The first, of course, is precautionary: put on a pair of gloves because some sexually transmitted diseases (including syphilis) can be acquired through simple skin abrasions. With gloves on, examine the penis by first palpating the shaft, and then by carefully looking for areas of induration or tenderness. Then, look for unusual curvatures (see Peyronie’s disease, question 47). Retract the prepuce to gain access to the glans, and inspect it for abnormalities. After completing the exam, return the foreskin to its original position since failure to do so may cause severe edema in unconscious patients. Finally, gently compress the glans between your thumb and forefinger to visualize the urethral meatus, and possibly express secretions. Note that this maneuver may be unyielding even in patients with a history of penile discharge. In this case, milk the shaft of the penis (from its base to the glans), since this may produce a few precious drops for analysis. Finally, examine the base of the penis for hair or skin abnormalities.
9 What is the cause of priapism?
Often idiopathic. Yet, priapism also may reflect systemic or local abnormalities:


10 And what about drugs?






11 What is phimosis?
From the Greek phimos (muzzle or snout), this is a narrowed opening of the prepuce, so that the foreskin cannot be retracted over the glans penis (Fig. 16-3). Usually congenital (from membranes binding the prepuce to the glans), phimosis also may result from acquired adhesions, often the sequela of poor hygiene, previous infections (chronic balanoposthitis), or a too-forceful retraction of a congenital phimosis. If untreated, it can degenerate into squamous intraepithelial cancer of the penis.

13 What is paraphimosis?
A condition related to, but actually different from, a phimosis. Once a phimotic prepuce is forcibly retracted over the glans, the edematous foreskin cannot be brought forward again, thus resulting in paraphimosis, a tight band of retracted foreskin behind the coronal sulcus (see Fig. 16-3). This is a very painful condition, which, if unrelieved, can cause urinary tract obstruction, venous engorgement, edema, and even necrosis of the foreskin and glans.
21 What kind of skin lesions can be seen on the penis?
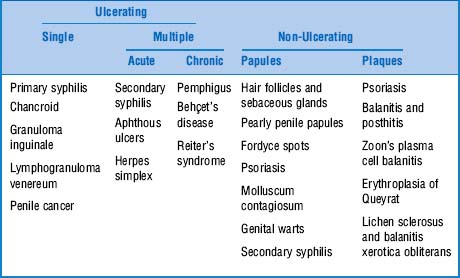
The most common are classified on the basis of appearance (Table 16-1):
1. Ulcerating: Skin craters filled with serum, pus, or crust. They represent a full-thickness loss of epidermis and can be single or multiple.
2. Non-ulcerating: Further divided into:


24 Describe the ulcerating lesion of chancroid
It is a painful, single ulcer, at times multiple, with lymphadenopathy.
26 Describe the ulcerating lesion of lymphogranuloma venereum
It is a small, nontender ulcer with unilateral tender lymphadenopathy.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


