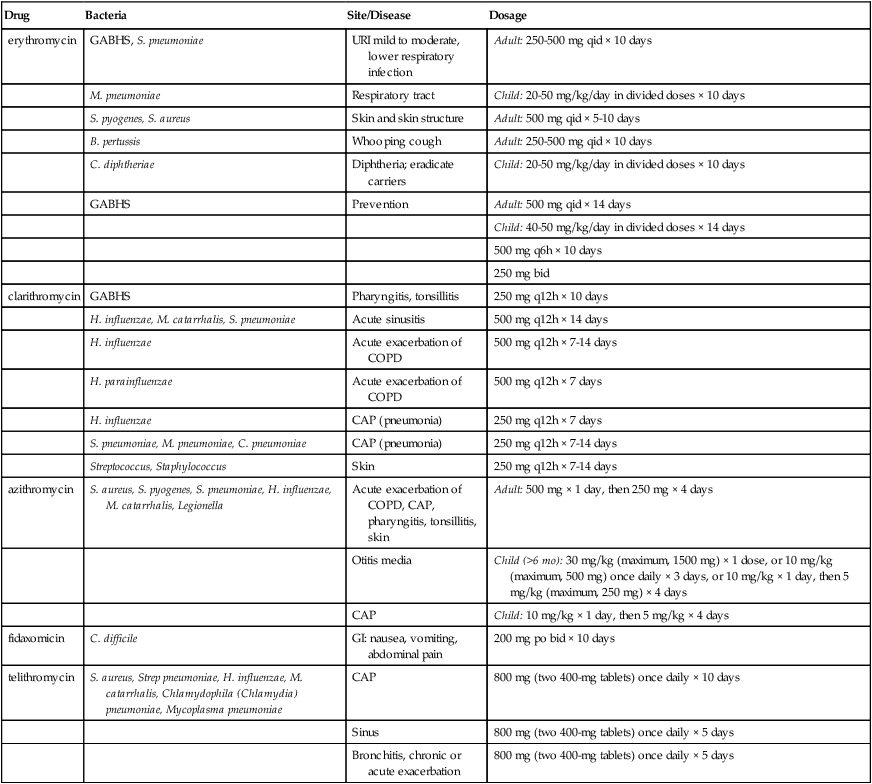
Chapter 62 INDICATIONS See Table 62-1 for specifics. TABLE 62-1 Macrolide Indications with Dosage and Administration Recommendations CAP, Community-acquired pneumonia; GABHS, group A β-hemolytic Streptococcus pyogenes.
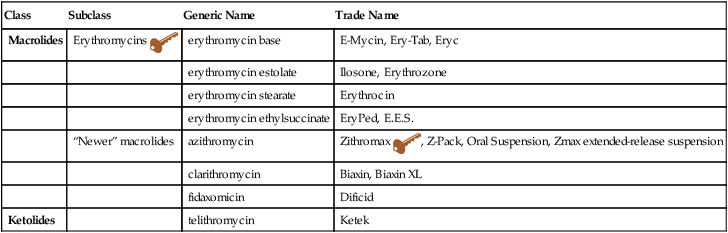
Macrolides
Class
Subclass
Generic Name
Trade Name
Macrolides
Erythromycins 
erythromycin base
E-Mycin, Ery-Tab, Eryc
erythromycin estolate
Ilosone, Erythrozone
erythromycin stearate
Erythrocin
erythromycin ethylsuccinate
EryPed, E.E.S.
“Newer” macrolides
azithromycin
Zithromax  , Z-Pack, Oral Suspension, Zmax extended-release suspension
, Z-Pack, Oral Suspension, Zmax extended-release suspension
clarithromycin
Biaxin, Biaxin XL
fidaxomicin
Dificid
Ketolides
telithromycin
Ketek
Drug
Bacteria
Site/Disease
Dosage
erythromycin
GABHS, S. pneumoniae
URI mild to moderate, lower respiratory infection
Adult: 250-500 mg qid × 10 days
M. pneumoniae
Respiratory tract
Child: 20-50 mg/kg/day in divided doses × 10 days
S. pyogenes, S. aureus
Skin and skin structure
Adult: 500 mg qid × 5-10 days
B. pertussis
Whooping cough
Adult: 250-500 mg qid × 10 days
C. diphtheriae
Diphtheria; eradicate carriers
Child: 20-50 mg/kg/day in divided doses × 10 days
GABHS
Prevention
Adult: 500 mg qid × 14 days
Child: 40-50 mg/kg/day in divided doses × 14 days
500 mg q6h × 10 days
250 mg bid
clarithromycin
GABHS
Pharyngitis, tonsillitis
250 mg q12h × 10 days
H. influenzae, M. catarrhalis, S. pneumoniae
Acute sinusitis
500 mg q12h × 14 days
H. influenzae
Acute exacerbation of COPD
500 mg q12h × 7-14 days
H. parainfluenzae
Acute exacerbation of COPD
500 mg q12h × 7 days
H. influenzae
CAP (pneumonia)
250 mg q12h × 7 days
S. pneumoniae, M. pneumoniae, C. pneumoniae
CAP (pneumonia)
250 mg q12h × 7-14 days
Streptococcus, Staphylococcus
Skin
250 mg q12h × 7-14 days
azithromycin
S. aureus, S. pyogenes, S. pneumoniae, H. influenzae, M. catarrhalis, Legionella
Acute exacerbation of COPD, CAP, pharyngitis, tonsillitis, skin
Adult: 500 mg × 1 day, then 250 mg × 4 days
Otitis media
Child (>6 mo): 30 mg/kg (maximum, 1500 mg) × 1 dose, or 10 mg/kg (maximum, 500 mg) once daily × 3 days, or 10 mg/kg × 1 day, then 5 mg/kg (maximum, 250 mg) × 4 days
CAP
Child: 10 mg/kg × 1 day, then 5 mg/kg × 4 days
fidaxomicin
C. difficile
GI: nausea, vomiting, abdominal pain
200 mg po bid × 10 days
telithromycin
S. aureus, Strep pneumoniae, H. influenzae, M. catarrhalis, Chlamydophila (Chlamydia) pneumoniae, Mycoplasma pneumoniae
CAP
800 mg (two 400-mg tablets) once daily × 10 days
Sinus
800 mg (two 400-mg tablets) once daily × 5 days
Bronchitis, chronic or acute exacerbation
800 mg (two 400-mg tablets) once daily × 5 days
< div class='tao-gold-member'>
Macrolides

 Key drug.
Key drug.Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


