CHAPTER 29 Lymphoma
Introduction
Peripheral blood (PB) and bone marrow (BM) are relatively frequently involved by lymphomas, particularly those with low-grade clinical behavior.1 BM aspiration and bone marrow trephine biopsy (BMTB) are currently performed at diagnosis as part of the staging of most patients with non-Hodgkin lymphomas (NHL) and in selected patients with Hodgkin lymphoma (HL). Criteria for patient selection for these procedures vary between treatment centers and are undergoing revision as techniques such as magnetic resonance imaging and positron emission tomography are refined to permit non-invasive assessment of disease spread. Evidence that BM involvement influences clinical outcome varies for different disease entities within the spectrum of lymphoproliferative disorders.2–9 BM involvement, and its extent, can be important factors in making clinical decisions concerning choice of treatment.
Lymphoproliferative diseases that present as leukemias have been considered elsewhere (see Chapter 28), as has plasma cell neoplasia (see Chapter 30). In this chapter, blood and BM involvement by lymphomas presenting primarily with lymph node or other solid organ involvement is discussed.
General comments on bone marrow (BM) examination in lymphoproliferative diseases
The full blood count, blood film, BM aspirate and BMTB have complementary roles in the investigation of BM involvement by lymphoma. In different lymphoproliferative diseases, each of these types of specimen may be of greater or lesser value.10–14 In lymphomas that do not readily display leukemic behavior, BMTB sections are frequently found to contain lymphoma when none is evident in the blood or BM aspirate.
Where circulating lymphoma cells are available in sufficient number in the peripheral blood (PB), these give the most consistent morphology and phenotyping by flow cytometry (FCM). BM aspiration without accompanying BMTB may be valuable if representation of disease in the PB is inadequate for diagnosis, permitting cytologic and immunocytochemical assessment of larger numbers of neoplastic cells. However, aspiration for the evaluation of BM involvement by lymphoma has a high false negative rate.13 Deposits of disease frequently occupy sites within the BM microenvironment that are suboptimally sampled by aspiration (e.g. paratrabecular zones). They may also be adherent to stromal components inducing focal fibrosis and less readily aspirated than BM hemopoietic elements. For these reasons BMTB in addition to aspiration is always recommended for the evaluation of BM involvement by lymphoma. Exceptionally, if BM aspiration alone is possible in some patients for whom BMTB cannot be performed, the aspirate films can still provide valuable information about hemopoietic reserve and iron stores. If aspiration proves technically difficult or a poor sample is obtained, BMTB should definitely be performed and an imprint or roll preparation made for cytologic assessment.
BMTB sections are used primarily for morphologic assessment, including analysis of the spatial distribution and extent of lymphomatous deposits.4,8–10,12,14–25 Spatial and cytologic assessment often provide clues to lymphoma subtype (e.g. the pattern of paratrabecular infiltration typical of follicular lymphoma) and can, as a minimum, be used to assess whether disease involvement represents indolent or agressive lymphoma. Histologic sections can also be used for immunohistochemistry (IHC), FISH and PCR; these additional investigations are particularly useful if PB or aspirated BM cells do not provide adequate representation of lymphoma. Where decalcification is employed in association with paraffin wax embedding of trephine cores, use of ethylene diamine tetra-acetic acid (EDTA) to decalcify by chelation, rather than acid exposure, offers excellent antigen and nucleic acid preservation.26–28 For immunophenotyping of lymphoid cell infiltrates in BMTB sections a similar, marginally more restricted, range of antibodies is employed to that used for FCM. Antibodies reactive with additional antigens such as CD79a, cyclin D1, IRF4/MUM1, PAX5 and Ki67 are also available which have been developed specifically for IHC use; these are referred to individually in the text that follows, where appropriate.
Differential diagnosis of reactive lymphoid aggregates vs lymphoma
Nodular aggregates of small lymphoid cells may be found in BMTB sections as a reactive phenomenon, unrelated to any neoplastic lymphoid proliferation. Criteria for distinguishing such aggregates from neoplastic lymphoid infiltrates remain imperfect and controversial.29–31 Immunostaining is helpful in only a minority of examples. Morphologic features remain the best guide, supported by application of molecular genetic techniques, such as PCR amplification and IGH/TCR rearrangement studies, in appropriately processed specimens. However, the sensitivity and specificity of the PCR methods employed may vary and the finding of a monoclonal IGH/TCR rearrangement cannot be assumed to equate with a diagnosis of lymphoma without other supportive evidence.32 In limited circumstances FISH performed using intact sections may be informative (consideration of t(11;14) and t(14;18), for example). For any techniques performed in addition to histological assessment of the original sections, there is a significant likelihood that small or few lymphoid aggregates will not be represented in the material available for testing.
To be accepted as reactive, lymphoid nodules should be few in number, centrally placed within intertrabecular spaces, small and round in profile with well-demarcated margins. A small capillary may be present, running from the periphery into the center of the nodule (Fig. 29.1) and there may be reactive changes such as aggregation of eosinophils in the adjacent hemopoietic tissue. An underlying meshwork of reticulin or CD23+ follicular dendritic cells may be present or absent, probably more dependent on the size of a particular nodule than on its reactive or neoplastic nature. The subjective nature of these criteria will be obvious to the reader but, to date, an objective gold standard for assessment of BM lymphoid nodules remains elusive.
The cytologic composition of lymphoid infiltrates is also critical to their interpretation. Most non-neoplastic aggregates consist of small lymphocytes with only occasional large blast cells; they show little evidence of plasma cell differentiation. Reactive germinal center formation is distinctly uncommon but, when it occurs, the composition of the lymphoid follicle recapitulates that found in lymph nodes and other organized lymphoid tissues. Formation of reactive germinal centers within BM lymphoid aggregates is said to be increased in patients with rheumatoid arthritis and other systemic chronic inflammatory disorders.32 Reactive lymphocytes, predominantly T-cells, also form a significant component of many granulomas in the BM, and the compact infiltrates of systemic mastocytosis; these lesions can be confirmed by IHC, if suspected, and should not be mistaken either for lymphoma or incidental reactive lymphoid nodules.
The laboratory investigation of blood and BM specimens suspected or known to have involvement by lymphoma
Blood
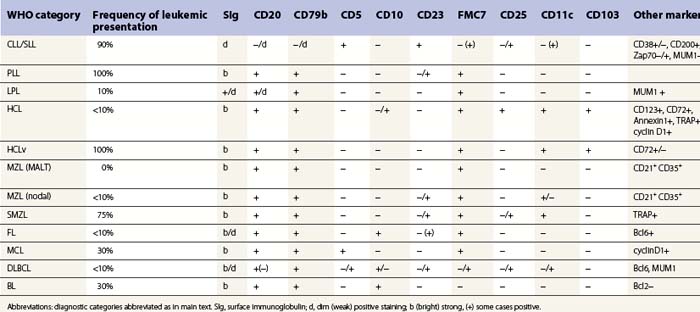
A full blood count and differential white cell count should always be performed. The blood film should be stained using May–Grünwald–Giemsa (MGG) or Wright’s method to assess cytologic features. When circulating abnormal cells are known or suspected to be present immunophenotyping by FCM should be performed; a useful basic antibody panel is shown in Table 29.1. PB cells should also be analyzed by classical cytogenetic and/or molecular genetic methods when the differential diagnosis includes lymphomas known to be associated consistently with abnormal genetic features.
Bone marrow aspirate
A minimum of three films should be prepared and air-dried, using MGG stain for cytologic assessment and differential cell count.33 A Perls stain is also desirable as a routine, for assessment of iron stores. Aspirated BM cells should also be sent in suspension for FCM immunophenotyping and genetic analysis.
Bone marrow trephine biopsy (BMTB)
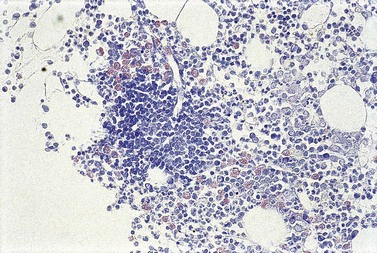
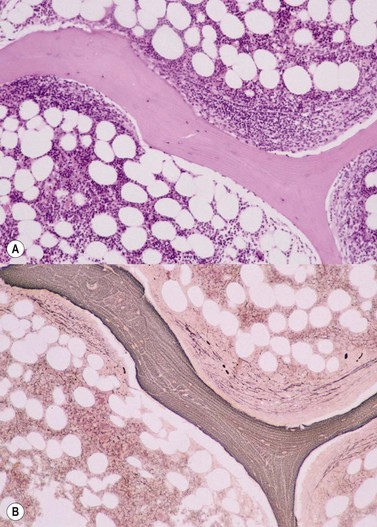
Cores of tissue should be collected that will contain at least 1 cm of interpretable, uncrushed BM after histologic processing. In practice, because of likely inclusion of cortex at the outer end and crushed tissue at the inner end, plus shrinkage that occurs during processing, unfixed cores at the time of collection should be at least 1.5 cm long10,34–36 If aspiration has been unsuccessful, touch preparations should be made using the trephine biopsy core by rolling it gently between two slides and then staining both air-dried slides with MGG. A detailed discussion of technical matters is beyond the scope of this chapter and only brief comments are made here. Further guidance can be found in references.26,37 Plastic-embedded specimens (usually in methyl or glycol methacrylate resin) require modifications to be made to standard tinctorial and IHC methods that may be difficult to incorporate into automated staining schedules but a wide range of immunostains can none the less be performed in laboratories specialized to handle these specimens. After processing the core for histology, thin sections (1–2 µm for plastic-embedded specimens; 3–4 µm for decalcified, paraffin wax-embedded ones) should be cut and stained with H&E from a minimum of three levels through the core. Levels are usually cut 25–50 µm apart, depending on local practice and the diameter of the specimen. On sections from the middle or deepest level, reticulin, PAS and Giemsa stains should be performed routinely. H&E provides a basic and familiar stain with which to assess cell morphology (Fig. 29.2A). Lymphoid infiltrates are often associated with increased reticulin deposition and a disturbance of the normal pattern of reticulin fiber distribution (Fig. 29.2B). PAS stain highlights carbohydrate-rich molecules and consequently stains immunoglobulin if it is of the IgM class and sufficiently abundant. IgM is richly glycosylated; consequently, intracellular and, occasionally, extracellular accumulation of this Ig can be detected in some cases of lymphoplasmacytic lymphoma (Fig. 29.3). The key importance of high-quality Giemsa staining in trephine biopsy sections cannot be over-emphasized (see Chapter 3). Any collection of lymphoid cells will stand out as being turquoise/blue in color, against a generally mauve/pink background (Fig. 29.1). IHC can be useful in confirming the precise diagnosis of lymphoma and in assessing its grade but is of limited value in differentiating reactive lymphoid aggregates in the BM from small deposits of low-grade lymphoma. For the latter task, molecular genetic analysis is gaining importance.30,32
The World Health Organization (WHO) classification of lymphomas
At the end of 1999, an outline version of a new lymphoma classification was published as a result of the WHO lymphoma classification project.38 This embodied the principles of the revised European–American lymphoma (REAL) classification,39 which was published in 1994 and has since become widely accepted in lymphoma diagnostic practice. A revision of the WHO classification was published in 2008 (Box 29.1).40
Box 29.1
Summary of the revised World Health Organization classification of lymphomas (2008)40
B-cell neoplasms
T- and NK-cell neoplasms
Immunodeficiency-associated lymphoproliferative disorders
(Italic text denotes entities regarded as provisional in the WHO 2008 Classification)
A novel and fundamental principle of the REAL classification was the definition of lymphomas according to their distinctive clinical, as well as pathologic, features. Much of the REAL classification remains little changed by the WHO, except for alterations in terminology, but considerable advances in the immunophenotypic and genetic contributions to defining lymphoma types have been incorporated. Some lymphomas considered as provisional entities in the REAL system became accepted as definite entities within the initial WHO classification, and this process, including the addition of new provisional entities, has continued with the 2008 revision. Box 29.1 summarizes the lymphoma categories recognized by the WHO 2008 scheme. Areas of uncertainty in lymphoma classification remain, however, and an important feature of the WHO classification is that it has flexibility to allow for further evolution in the understanding of hematological malignancies. An important advance in the WHO system over previous classifications is the recognition of subtypes of lymphoma that tend to exhibit leukemic behavior (see Chapter 28). Emerging information about the mutational status of immunoglobulin variable region genes in B-cell lymphomas41–46 and gene expresssion micro-array patterns across a wider spectrum of lymphomas,47–59 are likely to permit refinement of the classification as the biological significance of such data becomes clearer. However, while immunophenotypic, cytogenetic and molecular genetic features are central to the WHO classification, with expanded importance in the 2008 revision, little reference is made to the interpretation of patterns of BM involvement as a contribution to the definition of lymphoma entities.
Blood and BM involvement of lymphoma entities according to WHO classification
Description of entities primarily presenting as leukemias is provided in Chapter 28. Features of blood and BM involvement of lymphomas primarily presenting in lymph nodes or as extranodal infiltrates are described below.
Mature B-cell neoplasms
Lymphoplasmacytic lymphoma (LPL)
Clinical features, blood and bone marrow aspiration
Lymphoplasmacytic lymphoma is an indolent lymphoid neoplasm comprising 1–2% of all NHL.40,60–62 Studies in southern Europe have suggested an association between hepatitis C (HCV) infection and LPL,63–65 with treatment of the former being effective in controlling the lymphoma, but no similar association with HCV has been found elsewhere.
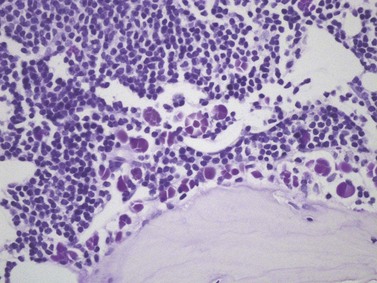
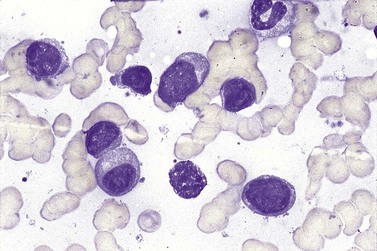
BM involvement is common at presentation and 30% of patients have splenomegaly and/or lymphadenopathy. The clinical presentation usually reflects the presence of a circulating paraprotein (IgM in almost all cases) with or without hyperviscosity symptoms. BM involvement by LPL with an IgM paraprotein underlies the clinical syndrome of Waldenström macrogobulinemia (see Chapter 30). There may be an associated peripheral neuropathy that is believed to be a paraneoplastic phenomenon.62 Pancytopenia may be present as a consequence of tumor burden such as BM failure or fibrosis. Blood involvement is rare, except in advanced disease; it is characterized by the presence in the circulation of plasmacytoid cells with an eccentric nucleus and basophilic cytoplasm. BM aspirate films show a mixture of small lymphocytes, lymphoplasmacytoid cells and mature plasma cells (Fig. 29.4). There is frequently an accompanying increase in mast cells. Typical immunophenotype findings are summarized in Table 29.1.
Bone marrow trephine biopsy
Bone marrow is frequently the predominant site of disease involvement in LPL. BMTB sections show infiltrates in most patients, often with more extensive involvement than suggested by aspirate films.10 The cells are predominantly small lymphocytes with varying numbers of plasma cells and cells having intermediate (plasmacytoid) features. The plasma cells may contain Dutcher bodies, which are inclusions of immunoglobulin that invaginate the nuclear membrane and appear intranuclear in histologic sections (Fig. 29.5). Less commonly, single or multiple intracytoplasmic immunoglobulin inclusions (Russell bodies) are found. Scattered lymphoid blast cells may be seen but true para-immunoblasts are absent and no proliferation centers are formed; finding the latter would indicate a diagnosis of B-cell chronic lymphocytic leukemia (B-CLL) with plasmacytic differentiation, rather than LPL. The presence of increased numbers of reactive mast cells in the marrow interstitium, sometimes located preferentially in the periphery of lymphoid infiltrates, may be helpful in supporting a diagnosis of LPL (Fig. 29.6). This phenomenon, however, is also seen in a minority of cases of CLL and is possibly related to IgM expression rather than to other properties of either disease.62,66 It has been suggested that mast cells contribute to B cell proliferation in LPL.67,68 The pattern of infiltration is usually irregular, paratrabecular or diffuse throughout the interstitium; mixtures of these patterns are common in individual cases. Well-defined nodular infiltrates are unusual and when nodules occur in LPL they are usually small and more elliptical or irregular than those seen in other small B-cell lymphomas. The paratrabecular infiltrates of LPL are not usually as extensive or regular as those found in follicular lymphoma. In some patients who have an IgM paraprotein, sinusoids contain PAS-positive proteinaceous material that represents plasma rich in IgM; there may also be interstitial and, rarely, intracytoplasmic deposition of crystalline PAS-positive IgM (Fig. 29.3). IHC shows that the small B-lymphocytes of LPL express CD19, CD20 (which may be weak or absent in cases with prominent plasma cell differentiation), CD79a and PAX5 but lack expression of CD5, CD10, BCL6 and cyclin D1. In occasional cases, a proportion of the neoplastic cells expresses CD23. Plasma cell differentiation is often evident with staining for CD79a and can be demonstrated more clearly using antibodies reactive with CD138 or IRF4/MUM1, or antibody VS38c that reacts with rough endoplasmic reticulum-associated p63 protein.69 Expression of monotypic immunoglobulin in the cytoplasm of cells showing plasmacytic differentiation is usually easily demonstrated, most commonly IgM kappa,40,70 and light chain mRNA production by such cells can also be shown by in situ hybridization (Fig. 29.7). Transformation to large cell lymphoma may occur but is not very common.
Genetic studies
Initial studies reporting a t(9;14)(p13;q32) IGH/PAX5 translocation in association with LPL70,70 have not been confirmed and no other consistent genetic associations have been identified. A variety of trisomies has been found, of unknown significance, and del(6q) may be associated with an adverse prognosis.71 Immunoglobulin heavy chain genes typically show hypermutation without evidence of ongoing acquisition of further mutations.72
Hairy cell leukemia (HCL)
Clinical features and pathology in the spleen
Hairy cell leukemia is a rare disease accounting for 2% of leukemias and predominantly affecting middle-aged men. The clinical presentation is with anemia, bleeding or infection (often with opportunistic organisms), reflecting PB cytopenias caused by hypersplenism and/or BM failure due to fibrosis associating tumor infiltrates.40 At presentation 60% of patients have splenomegaly and 40% hepatomegaly. In the spleen, HCL is recognized by the presence of a diffuse infiltrate of typical hairy cells (see below), causing effacement of normal red and white pulp architecture. As in the BM, splenic infiltration is accompanied by reticulin deposition, interstitial hemorrhage, sinusoidal vascular ectasia and peliosis-like disruption.73
Blood and bone marrow aspiration
Most patients with HCL have circulating hairy cells although numbers are typically low. These are medium-sized to large lymphoid cells which have abundant, weakly basophilic cytoplasm and hair-like projections from the cell surface.74 The nucleus is frequently indented and has a smooth chromatin pattern with indistinct nucleoli. Typical immunophenotyping results are summarized in Table 29.1. Peripheral cytopenias are common in HCL, particularly neutropenia and monocytopenia. BM aspiration is often unsuccessful due to increased marrow reticulin associated with HCL infiltration; when neoplastic cells are obtained, they are essentially identical in morphology to those found in PB. They may be accompanied by reactive mast cells and plasma cells. In touch preparations from BMTB, HCL cells may lack typical ‘hairy cell’ cytology but present as lymphatic cells with abundant cytoplasm.
Bone marrow trephine biopsy
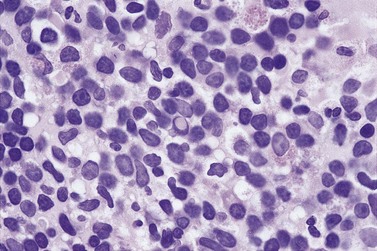
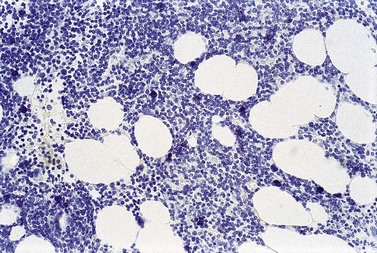
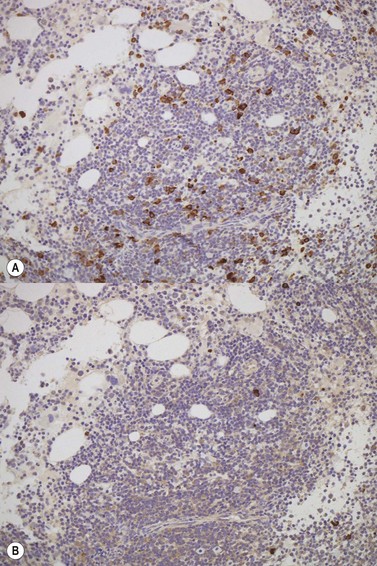
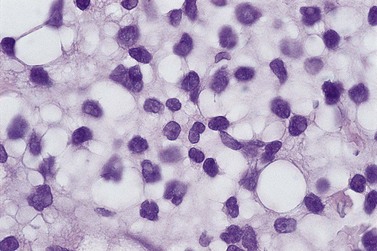
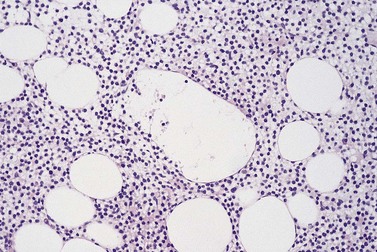
The degree of BM involvement is usually extensive at presentation, with large areas showing almost complete replacement of normal hemopoiesis by infiltrating hairy cells and partial or complete loss of fat spaces. Occasionally, the BM appears hypoplastic, with a subtle pattern of diffuse interstitial infiltration and partial preservation of hemopoiesis; granulopoiesis is often disproportionately reduced and this picture should not be confused with hypoplastic/aplastic anemia or a hypoplastic myelodysplastic syndrome (Fig. 29.8A). Subtle intrasinusoidal infiltration may also occur.25 CD20 staining is essential to determine the extent of infiltrates (Fig. 29.8B). In almost all cases of HCL, interstitial reticulin is greatly increased (Fig. 29.9), which is rarely the case in other hypoplastic states. The infiltrating cells are of medium size with round, oval or bilobed nuclei and abundant, empty-looking cytoplasm (Fig. 29.10). Occasionally, they appear spindle-shaped. The abundant cytoplasm gives an appearance of the cells being widely spaced from one another. Extravasation of red cells into the interstitium is common and sinusoids appear prominent, with gaping lumens, as a result of the background of increased reticulin fibers (Fig. 29.11). Collagen fibrosis is rare. Osteosclerosis may also occur rarely in association with HCL and may regress with treatment.75,76 Reactive mast cells are typically abundant throughout BM infiltrates and polytypic plasma cells may also be increased. Transformation of HCL to a more aggressive, large B-cell lymphoma occurs infrequently.77
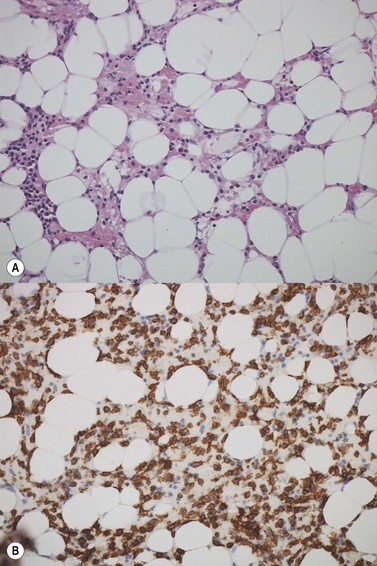

In BMTB sections, hairy cells can be shown by IHC to express CD20, CD79a and CD45RA but not CD5 or CD23. Expression of tartrate-resistant acid phosphatase (TRAP) can usually be demonstrated in extensive infiltrates78,79 although technical performance of anti-TRAP monoclonal antibodies varies and subtle HCL involvement may not be visible against background weak staining of hemopoietic cells. In many cases, hairy cells show heterogeneous, usually weaker than in mantle cell lymphoma, nuclear expression of cyclin D1 and, in a minority of cases, they are positive for CD10.80 Dot-like cytoplasmic expression of CD68 may also be seen. Hairy cells are strongly positive for CD25 and CD123. Hairy cells react well with the monoclonal antibody DBA44,79,81 which recognizes CD7282 a B-cell surface antigen strongly associated with hairy cells but not entirely specific. Annexin A1 and T-cell associated transcription factor T-bet offer further and, to date, highly specific additional markers for HCL.83,84
After treatment, HCL infiltration usually appears dramatically reduced and the increased reticulin resolves rapidly in most patients.75 Assessment of residual disease during and after therapy can be difficult in HCL, in which small interstitial clusters of scattered neoplastic cells may be all that remain; IHC usually reveals more disease than is readily apparent from standard tinctorial stains.
Genetic studies
Knowledge of genetic abnormalities associated with HCL is extremely limited and no consistent genetic associations have been found that appear causative. Immunoglobulin heavy chain genes are hypermutated but stable, without evidence of ongoing mutation. Partial understanding has been gained of genetic abnormalities underpinning the unusual properties of hairy cells;85 over-expression of the activator protein-1 (AP-1) transcription factor drives the expression of CD11c, resulting in some of the unusual stromal interactions and adhesive properties of HCL cells. Up-regulation of AP-1 is secondary to RAS activation in HCL which, in turn, may be due to reduced expression of RhoH that normally competes with Ras proteins at GTP binding sites. Reconstitution of RhoH expression in a mouse xenograft model of HCL reduced proliferation of neoplastic cells and prolonged survival.86
HCL variant (HCLv)
Clinical features and pathology in the spleen
HCLv is a rare disease with incidence of 3 cases per 1 000 000. It may be more common in Asian countries. It has been recognized as a provisional entity in the WHO 2008 classification;40 despite its name, it is clinically, immunophenotypically and genetically distinct from HCL.87,88 Patients typically present with splenomegaly; anemia is common but neutropenia and monocytopenia are rare. HCLv shows overlap between HCL and B-cell prolymphocytic leukemia (B-PLL) in their pattern of splenic involvement, with predominant diffuse red pulp involvement.40
Blood and bone marrow aspiration
There are usually abundant circulating neoplastic cells in HCLv with WBC usually in the range of 20–40 × 109/l. Although HCLv cells have cytoplasmic projections as in HCL, they are larger and have nucleoli more akin to those seen in B-PLL. BM aspiration is usually successful because HCLv is not associated with significantly increased reticulin fiber production in the marrow stroma. The immunophenotype of cells in HCLv is distinct from that found in HCL (see Table 29.1); they are generally negative for CD25, CD123 and annexin A1, with weak or absent TRAP expression. They show CD11c, CD103, FMC7 and strong sIg reactivity as in HCL.
Splenic marginal zone B-cell lymphoma (SMZL)
Clinical features and pathology in the spleen
This disease accounts for fewer than 2% of lymphoid neoplasms and occurs mainly in older individuals, affecting men and women equally.40 An association with hepatitis C has been noted in southern Europe.63
Within the spleen, there is widespread, generally uniform, involvement of the white pulp, giving a miliary appearance to the cut surfaces of splenectomy specimens.90 The germinal centers and mantles of white pulp nodules are atrophic and replaced by densely clustered small lymphoid cells surrounded by expanded marginal zones of more mixed composition. Cells in the marginal zones are predominantly slightly larger, lymphoplasmacytoid or monocytoid cells with more cytoplasm than the lymphocytes present centrally within involved nodules. Within the marginal zones there are also scattered immunoblast-like cells in varying proportions. Small satellite collections of marginal zone-type cells are frequently also present surrounding red pulp capillaries, and are often accompanied by small collections of epithelioid macrophages.73 There may be diffuse infiltration of red pulp cords and sinusoids by the small lymphoid cells. Appearances in splenunculi, when present, are identical to those in the main spleen; hilar lymph nodes show vaguely nodular replacement of follicles by small lymphocytes, usually without morphological evidence of marginal zone differentiation.
Blood and bone marrow aspiration
In PB, neoplastic cells in SMZL are slightly larger than normal lymphocytes, with a round nucleus and mature chromatin pattern. They have a relatively large volume of weakly basophilic cytoplasm and typically exhibit polar villi. BM involvement is almost always present and similar cells are usually readily apparent in aspirate. The immunophenotype (Table 29.1) shows usually positivity for CD19, CD20, surface IgM and in most cases IgD, no CD5 or CD10. CD23 and CD11c are positive in a fraction of cases. Cyclin D1 and Annexin A1 are negative.
Bone marrow trephine biopsy
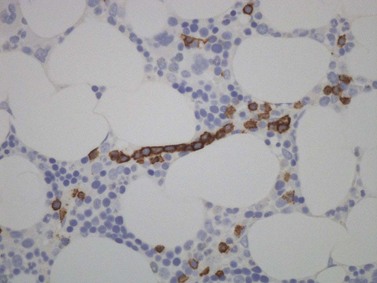
There is usually nodular, interstitial and, less regularly, paratrabecular infiltration by neoplastic cells.10,91 Intrasinusoidal infiltration is often an additional finding, demonstration of which may require IHC (Fig. 29.12). In occasional patients, a subtle and purely intrasinudoidal infiltrate may be present, requiring careful distinction from persistent polyclonal B-cell lymphocytosis (see below). A diffusely infiltrated, packed marrow is found only in rare patients.
Genetic studies
These neoplasms have clonally rearranged IgH and approximately 50% show hypermutation but evidence of ongoing acquisition of mutations is rare.92 Trisomy 3q has been found in a high proportion of cases, regarded as a late or secondary event in the neoplasm development and of uncertain biological relevance. The occurrence of translocations or allelic losses involving 7q31-32 and 7q21 is believed to be more significant. The latter result in dysregulation of CDK6.93 Microarray and CGH analysis suggests a distinctive profile involving up-regulation of gene expression within the AKT1 and B-cell receptor signaling pathways.94,95 Of note, t(11;18), found in a high proportion of MALT-type marginal zone lymphomas, is absent from SMZL.
Splenic diffuse red pulp small B-cell lymphoma
Clinical features and pathology in the spleen
This lymphoma has been introduced as a provisional entity in the 2008 revision of the WHO classification40 and has been described in patients predominantly of middle age and older, with men and women equally affected. Its clinical behavior is indolent.
Blood and bone marrow aspiration
Circulating lymphocytes often have villous processes and unusually basophilic cytoplasm.96 They may be present only in low numbers. Similar cells are present in BM aspirate. Their imunophenotype resembles that of SMZL but sometimes overlaps with HCLv and increasing experience of these two provisional entities may in future reveal genuine biological overlap between them.
Genetic studies
Hypermutation patterns of IGH and the spectrum of variable region gene usage differ from those found in SMZL and resemble HCL in some cases. A translocation, t(9;14), involving PAX5 and IGH has been found in some patients and genetic alterations associated with splenic, nodal and extranodal marginal zone lymphomas are absent.40,97
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT)-type
Clinical features and pathology at presenting sites
Extranodal marginal zone lymphomas of MALT-type are indolent lymphoproliferative disorders with a 10-year survival of more than 80%.60,61 The most common primary sites of MALT-type extranodal marginal zone lymphoma are within the gastrointestinal tract. Salivary glands, skin, orbit, lung and urogenital organs are the sites of origin in smaller numbers of patients. At presentation, 30% of patients have involvement of more than one mucosal site but lymph node spread is usually absent or localized to nodes close to the mucosal site(s) of involvement. As defined in the WHO classification, these lymphomas are low grade and arise in the context of normal or induced lymphoid tissue in the organs involved (e.g. that caused by infection with Helicobacter pylori in the stomach or Chlamydia psittaci in the orbit).40 The neoplastic cells are typically centrocyte-like, with a tendency to infiltrate epithelial structures and form lympho-epithelial lesions; they show monocytoid or plasmacytic differentiation to varying extents in different individuals.
Blood and bone marrow aspiration
Bone marrow involvement has been reported in 15–40% of cases.98 Fifteen per cent of patients are anemic at presentation but circulating lymphoma cells are not seen. Bone marrow aspiration rarely reveals the presence of lymphoma cells, even when BMTB shows histologic evidence of involvement. Immunophenotype is similar to other marginal zone lymphomas, as summarized in Table 29.1.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


