Lymphopenia is a common finding in the peripheral blood, and results from numerous different pathways (1, 2, 3, 4). Mechanisms of lymphocytopenia include impaired lymphopoiesis, increased apoptosis, and alterations in lymphocyte trafficking and homing. Apoptosis has been implicated in lymphopenia due to several different causes.
Many underlying conditions cause lymphopenia (Table 11.1) (5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23). Most patients with lymphopenia in a large general practice had a history of trauma, hemorrhage, bacterial or fungal sepsis, malignancies, cytotoxic therapy, human immunodeficiency virus and other viral infections, or organ transplantation.
Other reported conditions include those detailed in Table 11.1.
Laboratory studies show an automated absolute lymphocyte count below the lower limit of normal. This value varies depending on the age of the patient and and the laboratory’s own data. In our laboratory, the lower limit of normal ranges from 4.0 × 109‘L in children from 3 months to 2 years of age, depending on the specific age, and 0.850 × 109‘L in adults. Flow cytometry reveals decreases in B cells, T cells, and’or natural killer (NK) cells. The peripheral blood shows lymphopenia without specific morphologic alterations.
CD4-Positive T-Cell Lymphopenia
CD4-positive T-cell lymphopenia is usually due to infection by retroviruses. The predominant organism is human immunodeficiency virus-1 (HIV-1), the agent of acquired immunodeficiency syndrome (AIDS). However, CD4 lymphopenia also occurs in patients infected with HIV-2, human T-cell lymphotropic virus-I (HTLV-I) and HTLV-II. There remain some cases not accounted for by infection with these viruses, termed idiopathic CD4 T-cell lymphopenia.
Idiopathic CD4-positive T lymphocytopenia (ICL) is defined as a CD4-positive T-cell count less than 0.3 × 109‘L or less than 20% of the total T-cell count on two occasions in the absence of any immunodeficiency disorder or therapy (24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34). The mechanism of this lymphocytopenia is unknown. In one case, autoantibodies against CD4-positive T cells were documented.
Patients present with opportunistic infections and with severe or disseminated infection by common pathogens. Autoimmune diseases may be present, such as alopecia areata, Sjögren syndrome, and vitiligo. Malignant lymphomas, including primary effusion lymphoma, and other malignant tumors have been described in these patients.
The peripheral blood shows lymphopenia without morphologic abnormalities. No specific bone marrow findings have been reported.
Bone Marrow Lymphopenia
Relatively few studies of bone marrow lymphopenia have been done. NK cells are reduced in the bone marrow of patients with aplastic anemia (35).
REACTIVE LYMPHOCYTOSIS
Peripheral Blood Lymphocytosis
Peripheral blood lymphocytosis occurs under many conditions, as seen in Table 11.2 (36, 37, 38, 39, 40). In some cases, no etiology is apparent.
The peripheral blood smear may show unremarkable lymphocytes, lymphocytes with cleaved or convoluted nuclei, atypical lymphocytes, and’or immunoblasts. Genetic studies usually reveal no clonal abnormalities. However, oligoclonal and monoclonal populations have been reported in some cases, without other signs of clinical progression or malignant transformation. Specific clinicopathologic entities are further described below.
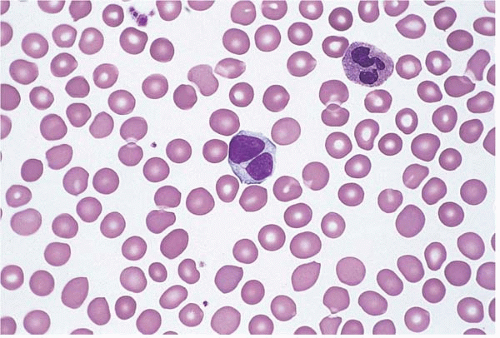
Persistent polyclonal B-cell lymphocytosis is a rare disorder, usually found in young to middle-aged female cigarette smokers (Fig. 11.1) (41, 42, 43, 44, 45, 46, 47). It is associated with a polyclonal increase in serum immunoglobulin M level, serologic evidence of previous or chronic active Epstein-Barr virus infection, functional B-cell and T-cell abnormalities, and HLA-DR7 phenotype. The peripheral blood characteristically shows binucleated lymphocytes. Flow cytometry shows polyclonal, CD5-positive B cells. The bone marrow may also show lymphocytosis, including intravascular involvement. Genetic studies have demonstrated clonal abnormalities in some cases, especially +i(3q) and clonal immunologic gene rearrangement, as well as other abnormalities indicative of chromosomal instability. Evolution to malignant lymphoma has rarely been reported. The differential diagnosis includes malignant B-cell lymphoma.
TABLE 11.1 Conditions Associated with Peripheral Blood Lymphopenia
Nonneoplastic Conditions
Acute pancreatitis
Aging
Apheresis for hematopoietic stem cell donation
Aplastic anemia
Autoimmune disorders
Bacterial or fungal sepsis
Chronic renal failure
Common variable immunodeficiency
Congenital immunodeficiency syndromes
Corticosteroid therapy
Cytotoxic therapy
Ethanol abuse
Hemorrhage
Human immunodeficiency virus and other viral infections
Idiopathic CD4-positive T-cell lymphopenia
Lymphangioma
Nutritional deficiencies
Organ transplantation
Posttransplantation lymphoproliferative disorder
Sarcoidosis
Stem cell transplantation
Stress
Trauma
Neoplastic Conditions
Myeloproliferative disorder
Myelodysplastic syndrome
Malignant lymphoma
Malignant thymoma
Other malignancies
Polyclonal hairy B-cell lymphoproliferative disorder is an unusual entity, reported in Japanese women with persistent lymphocytosis (48, 49, 50, 51). Laboratory studies show polyclonal hypergammaglobulinemia and polyclonal B-cell lymphocytosis, sometimes accompanied by cytopenias. The morphologic features are similar to hairy cell leukemia. The etiology is unknown.
Hyperreactive malarial splenomegaly is another type of chronic B-cell lymphocytosis (52, 53, 54, 55, 56). Genetic studies have revealed clonal immunoglobulin gene rearrangement in some, supporting an etiologic relationship between hyperreactive malarial splenomegaly and splenic marginal zone lymphoma.
TABLE 11.2 Conditions Associated with Reactive Peripheral Blood Lymphocytosis
Nonneoplastic Conditions
Anaphylactic shock
Autoimmune and connective tissue disorders
Common variable immunodeficiency
Connective tissue disease
Drug hypersensitivity reaction
Exercise
Graft-versus-host disease
Human immunodeficiency virus-related diffuse lymphocytosis syndrome
Hyperreactive malarial splenomegaly
Hyperthermia
Infection
Kikuchi disease
Mosquito bite hypersensitivity
Persistent polyclonal B lymphocytosis
Sickle cell crisis
Splenectomy
Stem cell transplantation
Stress
Toxic industrial exposure
Trauma
Neoplastic Conditions
Invasive thymoma
Other malignancies
Other cases of clonal and nonclonal chronic B-cell lymphocytosis have been reported in children and in patients with chronic hepatitis C infection, aging adults, and patients with a family history of chronic lymphocytic leukemia (57, 58, 59, 60, 61, 62, 63, 64, 65, 66). The clonal populations may be transient or stable. They are usually small, and are of uncertain clinical significance.
Figure 11.1 Persistent polyclonal B lymphocytosis, peripheral blood. A binucleated lymphocyte is seen in this specimen from a young woman who was a cigarette smoker.
TABLE 11.3 Conditions and Infectious Agents Associated with T-Cell Lymphocytosis
Nonneoplastic conditions
Aging
Ataxia telangiectasia
Autoimmune disease
Benzene toxicity
Borrelia burgdorferi
Common variable immunodeficiency
Cytomegalovirus
Epstein-Barr virus
Erythroderma
Graft-versus-host disease
HIV-1
HTLV-1
Pure red cell aplasia
Rheumatoid arthritis
Stem cell transplantation
Neoplastic conditions
Chronic B-cell lymphocytic leukemia
Hairy cell leukemia
Hodgkin lymphoma
Plasma cell (multiple) myeloma
Invasive thymoma
Clonal and nonclonal T-cell lymphocytosis has been reported in numerous settings (Table 11.3) (67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93). Clonal populations may be transient or persistent but do not show signs of malignant progression. T-cell lymphocytosis may precede the diagnosis of invasive thymoma by years and may persist after resection of the tumor.
The peripheral blood shows absolute lymphocytosis composed of small lymphocytes or large granular lymphocytes. Flow cytometry shows an increase in T-cells expressing CD8, CD4, both CD4 and CD8, or neither. Either T-cell receptor (TCR) α’β or TCR γ’δ may be expressed. Genetic studies may demonstrate polyclonal, oligoclonal, or monoclonal populations.
Diffuse infiltrative lymphocytosis syndrome is a complication of human immunodeficiency virus-1 infection (94, 95, 96, 97). This disorder is characterized by lymphocytosis of the peripheral blood, nerves, salivary glands, and other organs. Flow cytometry reveals an activated CD8-positive T-cell phenotype, with expression of CD3, CD8, CD11c, CD57, and HLA-DR, but not CD4, CD16, or CD56. Genetic studies may show polyclonal, oligoclonal, or monoclonal TCR gene rearrangement. Clonality is apparently caused by expansion of one or more human immunodeficiency virusspecific clones with restricted TCR gene use. The disorder has become less common with the introduction of highly active antiretroviral treatment.
Natural killer cell lymphocytosis has been reported in patients with Epstein-Barr virus infection, other infectious diseases, mosquito bite hypersensitivity, peripheral neuropathy, Sjögren syndrome, splenectomy, and clonal T-cell large granular lymphocytosis (63,98, 99, 100, 101, 102, 103, 104, 105, 106). The peripheral blood shows increased large granular lymphocytes indistinguishable from CD8-positive cytotoxic T cells.
Only gold members can continue reading. Log In or Register to continue