Needle aspiration of lymph nodes is one of the oldest applications of the technique in the diagnosis of human disease. In 1904, two British military surgeons, Greig and Gray, working in Uganda, published a paper describing the diagnosis of sleeping sickness by recognizing mobile trypanosomes in lymph node aspirates. In 1921, Guthrie of Johns Hopkins described the application of needle aspiration to the diagnosis of tumors. In 1930, Martin and Ellis of Memorial Hospital for Cancer (now the Memorial Sloan-Kettering Cancer Center) included tumors that had metastasized to the lymph nodes among the targets of aspiration biopsy.
As a result of the pioneering work of Franzén et al (1960) and the widespread current acceptance of the technique, aspiration of lymph nodes has become a standard laboratory procedure.
The spectrum of applications of fine needle aspiration (FNA) biopsy in diagnosing disease has become ever wider. Although metastatic cancer is still the most common target of lymph node aspiration, a large number of benign disorders have been identified using the procedure. Applications of immunologic techniques now allow a secure identification of a broad spectrum of primary malignant lymphomas.
ANATOMY AND HISTOLOGY OF LYMPH NODES
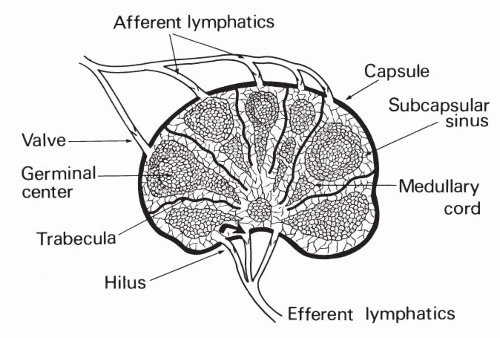
A lymph node may be conceived of as an encapsulated spongy sieve, filtering and modifying the lymphatic fluid between the points of entry and exit. The normal lymph node is bean-shaped, with lymph entering the node through the afferent lymphatics, piercing the convex surface of the capsule, and exiting through the efferent lymphatics in the hilus, which is an area of indentation in the concave side of the node. The principal component of the lymph node is lymphoid tissue, which is normally distributed in an orderly fashion within compartments that are constructed of connective tissue and circulatory sinuses (Fig. 31-1).
A connective tissue capsule encloses the lymph node, which is further subdivided into anatomic compartments by a number of connective tissue trabeculae that extend from the convex aspect of the capsule to the hilus. The capsule and the trabeculae provide the framework for a series of circulatory channels or sinuses, which are lined by endothelial cells and are filled with lymph fluid and the cells carried within it.
Figure 31-1 Diagrammatic presentation of lymph node structure.
The following brief overview of lymphocyte classification is cited merely in support of the anatomic data. There are two principal families of lymphocytes, the thymusderived (T) and bursa- or bone marrow-derived (B) lymphocytes. Although the significance of this classification is not discussed at length here, a principal function of the B lymphocytes and derivative cells, such as plasma cells, is the formation of immunoglobulins, which confer humoral immunity, whereas T lymphocytes play a major role in cell-mediated immunity. Complex interactions are now known to exist between the B and T lymphocytes and their subsets. Lymphocytes without obvious B or T characteristics have been designated, in the past, as null cells. With the use of additional markers, these cells can now be classified as either B or T or their subtypes. Classes of dendritic follicular cells that may interact with lymphocytes by processing antigens are also present in lymph nodes; they populate sinusoidal, stromal, and T and B areas.
The distribution of the B and T cells in a normal lymph node is orderly and follows anatomic divisions. Three regions of the lymph node can be distinguished: the cortex, which is situated beneath the capsule; the medulla, which is close to the hilus; and the intermediate paracortex, which is located between the capsule and hilus. The cortex and medulla represent zones of B cells, whereas the paracortex represents a zone of T cells.
The cortex contains the majority of lymphatic nodules (follicles) which, during postnatal life, usually contain germinal centers. As a consequence of antigenic stimulation, the small B-lymphocytes within the germinal centers are transformed into large cells that have large, round nuclei and prominent nucleoli. Previously known as reticulum cells, these large cells have been designated by Lukes and Collins (1974) as large noncleaved cells and by Lennert (1967) as centroblasts. The transformation of the small lymphocytes into the large noncleaved cells proceeds through several stages and forms, identified by Lukes and Collins (1974) as small cleaved cells, large cleaved cells, and small noncleaved cells. The large noncleaved cells may participate in further lymphopoiesis or transform into immunoblasts which, outside of the germinal centers, evolve into plasma cells. Cumulatively, the transformed lymphocytes may be designated as follicle center cells. The germinal centers also harbor macrophages that usually contain fragments of phagocytized material in their cytoplasm (tingible body macrophages), and the nonphagocytic dendritic reticulum cells that have pale vesicular nuclei, tiny nucleoli, and abundant, ill-defined cytoplasm.
The paracortex contains small T-type lymphocytes that are suspended in nests composed of interdigitating reticulum cells. Under antigenic stimulation, the T-type lymphocytes may evolve into T-type immunoblasts.
The medulla is composed of small B-type lymphocytes that are packed tightly in sheets and cords separated by medullary sinuses. The lymph nodes also contain cells previously known as null cells that do not appear to be assigned to any specific anatomic compartment but are either of B or T derivation. Dendritic cells are dispersed among the various elements of the lymph node and are active in presenting antigens to the lymphocytes. These cells have cytoplasmic extensions (“dendrites”) and may express keratin.
Immunologic techniques, described in this chapter and in Chapter 45, are required to identify the different types of lymphocytes because they cannot be distinguished from each other by light microscopic features, either in histologic sections or in cytologic smears.
Normal children and young adults have well-developed lymph nodes with numerous follicles. A reduction in the number of lymph follicles is common in the elderly. A regression of lymphoid tissue may also be observed, with replacement either by fat, for example, in the axillary lymph nodes, or by connective tissue, as observed in the inguinal lymph nodes.
FINE-NEEDLE ASPIRATION BIOPSY TECHNIQUE
Aspiration biopsy should be limited to enlarged lymph nodes that are either superficial and palpable or deep and visualized using a radiologic or ultrasound technique. The aspiration of palpable lymph nodes should be performed by a person familiar with the principles of this technique, discussed in Chapter 28. After cleansing of the skin, palpable lymph nodes should be immobilized between the fingers of one hand before the aspiration is performed with the dominant hand. Otherwise, the tip of the needle may displace the target, resulting in an inadequate specimen.
For routine aspirations, air-dried, methanol-fixed smears stained with a variant of the Romanovsky hematologic stain (May-Grünwald-Giemsa or Diff-Quik) and alcohol-fixed smears stained with Papanicolaou should be made.
Preliminary Assessment of Smears
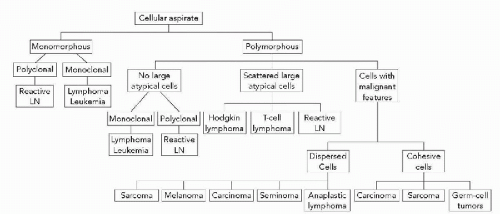
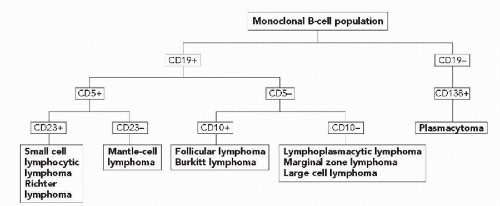
The first task in evaluating a smear from a patient with lymphadenopathy is to assess its compositions and cellular features. The cell population may be polymorphous, containing a mixture of cell types, or monomorphous, containing one predominant cell type. A schematic outlines the differential diagnosis of polymorphous (Fig. 31-2) and monomorphous (Fig. 31-3) populations.
Figure 31-2 Assessment of cells in lymph node (LN) aspirate.
An important index of the presence of lymphocytes in smears is the presence of lymphoglandular bodies, first observed by Downey and Weidenreich (1912) and subsequently recognized as an important diagnostic landmark by Søderstrøm in his book published in 1966. The lymphoglandular bodies (also known as Søderstrøm bodies) are approximately spherical, small, pale, basophilic fragments of cytoplasm that are best observed against the background of air-dried, MGG-stained smears of lymph nodes or bone marrow (Khoory, 1983; Flanders et al, 1993; Francis et al, 1994). The importance of lymphoglandular bodies in the diagnosis of malignant lymphoma is described in the next section.
Further Evaluation of Samples
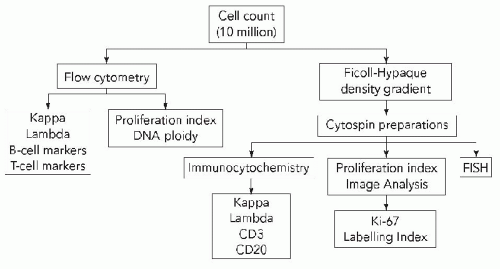
Depending on the results of the initial cytologic evaluation and the clinical history, appropriate ancillary studies can be performed (Fig. 31-4). An adequate portion of the aspirate should always be saved in tissue culture medium or another transport medium. It is helpful to count the saved cells to determine whether the sample is adequate for ancillary studies. If an infectious process is suspected, then material should be obtained for microbiologic culture and special stains for microorganisms (e.g., Gomori’s methenamine silver, Ziehl-Neelsen, Gram stains).
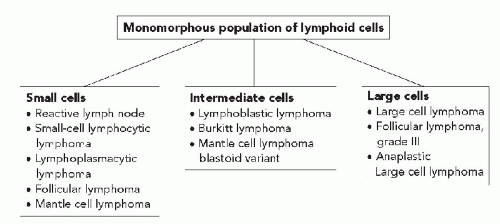
Figure 31-3 Differential diagnosis of a monomorphous lymphoid population based on cell size.
Our approach to the work-up of suspected lymphoproliferative disorders consists of the following steps:
Immunophenotyping is performed with flow cytometry or immunocytochemistry on cytospin preparations (Sneige et al, 1990; Katz et al, 1993a). In the initial workup of a lymphoproliferative disorder, an optimal flow cytometry panel includes antibodies to kappa, lambda, CD3, CD5, CD10, CD19, CD20, and CD23 antigens, coexpression of CD19 and CD5, and coexpression of CD19 and CD10. For explanation of the significance of these antibodies see Chapters 5, 47, and the discussion of lymphomas below. This panel is useful in classifying most of the lymphomas and can be modified depending on the differential diagnosis (Fig. 31-5). A limited panel consisting of kappa and lambda to determine clonality, a T-cell marker (CD3), and a proliferation marker (Ki-67) can be performed if the patient has a previous diagnosis of lymphoma and the cytomorphologic features correlate with that diagnosis.
DNA ploidy analysis is used to analyze the proportion of cycling cells by image analysis, flow cytometry, or immunostaining with Ki-67 (Katz et al, 1993b; 1993c).
Genotyping is performed only in the rare cases of nonmarking lymphomas, low-grade T-cell lymphomas, lymph nodes partially involved by lymphoma, or equivocal marker studies (Katz et al, 1991).
Figure 31-4 Schema for evaluation of lymphocyte-rich aspirate in cases suspected of a lymphoproliferative disorder.
NONNEOPLASTIC LYMPH NODES
The principal indication for FNA is persistent enlargement of lymph nodes, and the purpose of the procedure is to establish causes of lymphadenopathy that cannot be reliably diagnosed on clinical grounds (Table 31-1). Such nonneoplastic conditions as inflammation, infection, autoimmune disorders, and hypersensitivity reactions are associated with lymphadenopathy (Dorfman and Warnke, 1974; Koss et al, 1992).
Figure 31-5 Use of immunophenotyping in the differential diagnosis of B-cell neoplasms.
Acute Lymphadenitis
Clinically, acute lymphadenitis usually appears as a red, hot, tender area. Superficial lymph nodes that drain a dental abscess, an inflamed appendix, a tubo-ovarian abscess, or an infected wound are typically affected. The most common causes of acute lymphadenitis are bacteria or their toxic products.
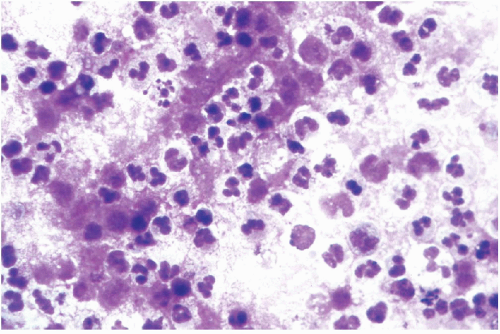
Early in the disease process, lymph node aspirates contain an admixture of neutrophils and lymphocytes. Later, the aspirates contain a purulent material composed of neutrophils and cellular debris (Fig. 31-6). As the acute inflammatory process subsides, neutrophils are admixed with plasma cells and large macrophages containing fragments of phagocytized material, known as tingible body macrophages. The aspirated material can be sent for bacterial culture. Although Gram staining can be performed on aspirates, the results may be difficult to interpret, especially on smears that are destained and restained.
Chronic lymphadenitis, more often referred to as reactive hyperplasia of lymph nodes, is the most common cause of lymphadenopathy and the most common diagnosis made on lymph node aspirates.
Lymph node enlargement in chronic conditions may be caused by an enlargement of the lymphoid follicles, the pulp of the lymph nodes, the peripheral sinuses, or a combination of all three. In reactive hyperplasia, one component of the lymph node usually predominates and, therefore, the disorder is usually classified by pattern (Table 31-2). However, the architectural pattern cannot be assessed by FNA and, therefore, it is difficult to determine specific causes of benign hyperplasia in a cell sample.
Follicular and Paracortical Hyperplasia
Follicular hyperplasia can occur at any age, but it is more common in children. The cervical, axillary, and inguinal lymph nodes are frequently involved because they drain large areas of the body. Reactive nodes are usually less than 3 cm in diameter, although they may be larger in children.
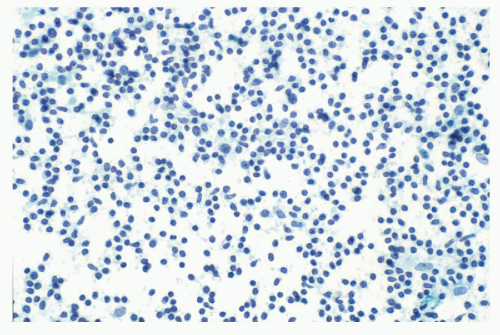
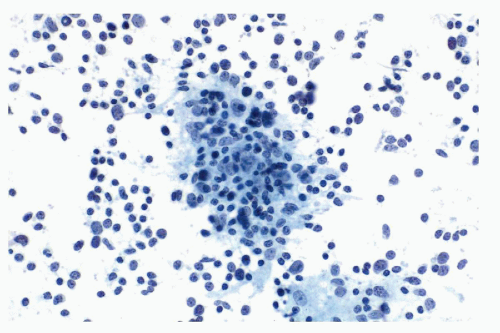
In general, the aspirates are quite cellular and are composed of dispersed, isolated, single cells with marked variability in size and configuration. Small lymphocytes are usually the dominant cell type (Fig. 31-7). Follicle center cells, which are a mixture of small and large lymphocytes with cleaved nuclei, large cells with vesicular nuclei, and immunoblasts, are present in varying proportions, sometimes forming small cell aggregates (Fig. 31-8). In optimal preparations, one may be able to differentiate between large noncleaved cells (centroblast) containing two or three nucleoli located near the nuclear membrane and immunoblasts containing only one centrally placed, often irregular, large nucleolus (Koss et al, 1992). Plasma cells and tingible body macrophages are usually present, the latter recognized by their very large size and the presence of phagocytized debris in their vacuolated cytoplasm (Fig. 31-9). Dense, basophilic fragments of apoptotic nuclei and occasional mitotic figures may be seen.
Immunophenotyping reveals a typical polyclonal population with no clonal excess of light chains (Fig. 31-10). Reactive T cells may constitute a large proportion of the cell population; however, if they exceed 80%, a low-grade T-cell lymphoma should be considered. DNA ploidy analysis usually shows a diploid population with variable S-phase.
Conditions Associated with Follicular and Paracortical Hyperplasia
Rheumatoid arthritis is an autoimmune disease that is associated with lymphadenopathy. In rheumatoid arthritis, aspirates show florid, reactive hyperplasia and numerous plasma cells with eosinophilic, cytoplasmic inclusions, known as Russell bodies. Similar changes can be seen in lymph nodes from patients with Sjögren syndrome, characterized by keratoconjunctivitis and xerostomia, and Felty syndrome, characterized by splenomegaly, hematologic disorders that result from hypersplenism, leg ulcers, and polyarticular rheumatoid arthritis.
Systemic lupus erythematosus (SLE) is also associated with lymphadenopathy. Aspirates taken from patients with SLE show numerous small lymphocytes, transformed lymphocytes, and tingible body macrophages in a background of necrosis. In addition, LE cells in various stages of formation may be observed. The LE cells contain amorphous basophilic bodies, composed of aggregates of DNA, polysac-charides, and immunoglobulins, and ranging from 5 to 12 microns in diameter (Ko and Lee, 1992; see Chap. 26).
TABLE 31-2 CONDITIONS ASSOCIATED WITH REACTIVE LYMPHOID HYPERPLASIA: PREDOMINANT HISTOLOGIC PATTERN BY ETIOLOGY
Figure 31-7 Reactive lymph node. Smears show predominantly small cleaved lymphocytes and occasional noncleaved cells.
Castleman disease is also known as giant lymph node or angiofollicular hyperplasia. There are two morphologic subtypes: the more common hyaline-vascular and the less common plasma cell variant. The hyaline-vascular type can affect patients of any age, but most are asymptomatic young adults. The mediastinum is most commonly involved, followed by the cervical lymph nodes. Aspirates taken from patients with the hyaline-vascular form of Castleman disease show primarily small, mature lymphocytes and occasionally larger, atypical cells consistent with follicular dendritic cells. Capillaries are often intermixed with the lymphocytes and reticular cells (Hidvegi et al, 1982; Meyer et al, 1999).
Figure 31-8 Reactive lymphoid hyperplasia. The field shows a lymphoid aggregate containing follicular center cells.
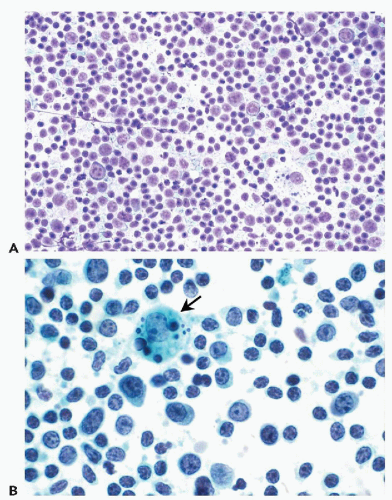
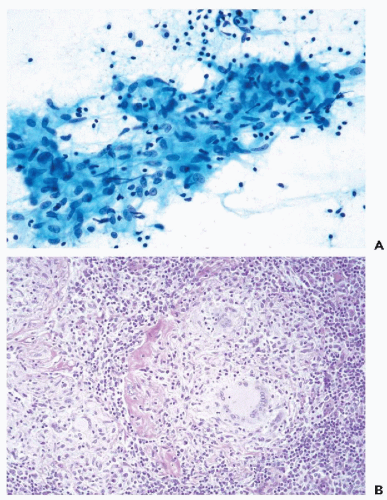
Figure 31-9 Reactive lymphoid hyperplasia. Aspirate shows a polymorphous population composed of small and large cleaved cells, plasmacytoid lymphocytes, and tingible body macrophages (arrow) (A: Diff-Quik stain, low magnification; B: Papanicolaou stain, high magnification.)
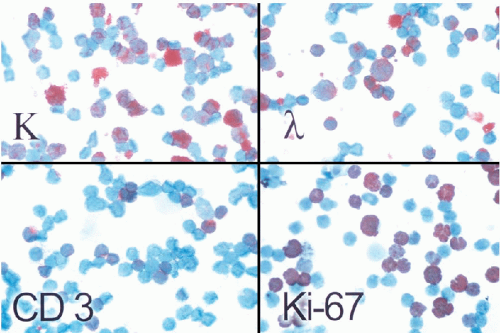
Figure 31-10 Reactive lymphoid hyperplasia. Immunocytochemical studies show a polyclonal B-cell population comprising a mixture of kappa- and lambda-positive cells and scattered T-cells (CD3+). There is an elevated proliferative activity with a labeling index of 30% with Ki-67 antibody consistent with a reactive process (Immunoperoxidase stain.)
The plasma cell variant of Castleman disease may be localized or multicentric. The localized form tends to affect the mediastinum and the intraabdominal lymph nodes. Patients are usually young adults who have systemic symptoms such as fever, anemia, and hypergammaglobulinemia. The multicentric form is more common in patients who are middle-aged or older and who have peripheral lymphadenopathy; they tend to have more severe systemic symptoms than patients with the localized form. Multicentric Castleman disease may also occur in human immunodeficiency virus (HIV)-infected individuals in whom it is associated with human herpesvirus type 8 (Kaposi sarcoma virus). Aspirates show a polymorphous lymphoid population with occasional immunoblasts and higher than normal numbers of plasma cells, some of which contain Russell bodies.
Kikuchi lymphadenitis is a self-limited disease of unknown cause that appears to be more prevalent among Asians than Western populations. Most patients are young women who have painful unilateral cervical lymphadenopathy. Infrequently, the lymphadenopathy is generalized. Histologically, there are localized areas of necrosis in cortical or paracortical areas with prominent karyorrhexis but no polymorphonuclear infiltrate. Atypical mononuclear cells and immunoblasts are on the periphery. Some patients have hematologic abnormalities.
Smears taken from such patients show a heterogeneous population of small and large transformed lymphocytes and tingible body macrophages. Scattered in the background are necrotic debris and karyorrhectic (apoptotic) cells (Kung et al, 1990; Hseuh et al, 1993; Tsang et al, 1994).
Kimura disease is a chronic inflammatory disorder of unknown origin that may be an aberrant immune reaction to an unknown stimulus. This disease is more prevalent in men than in women among Asian populations. Patients often have painless lymphadenopathy of the head and neck region with cutaneous or subcutaneous nodular lymphoid infiltrates. Aspirates are consistent with florid reactive lymphoid hyperplasia with Warthin-Finkeldey-type multinucleated giant cells (Fig. 31-11) and eosinophils (Hui et al, 1989).
Dermatopathic Lymphadenopathy
In the presence of chronic skin disorders, lymph node enlargement is common. Histologically, there is follicular and paracortical hyperplasia and accumulation of phagocytized granules of melanin. Pigment from tattoos may mimic melanin accumulation (Zirkin et al, 2001). The principal cells involved are the interdigitating reticulum cells that may show complex nuclear contours (Asano et al, 1987).
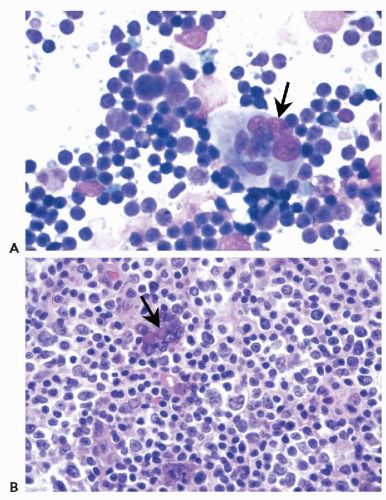
Figure 31-11 Kimura disease.A. Aspirate shows a polykaryocyte (Warthin-Finkledey cell [arrow]) in a polymorphous lymphoid background. B. Tissue section also shows a germinal center also with a polykaryocyte (arrow). (A: Diff-Quik stain.)
The most important points of differential diagnosis are: lymphadenopathy associated with cutaneous T-cell lymphoma (see below) and metastatic malignant melanoma (Burke et al, 1986; Cangiarella et al, 2000).
Viral Infections
Virus infections, such as with the Epstein-Barr virus (EBV) and the human immunodeficiency virus (HIV), are usually associated with lymphadenopathy. Occasionally, cytomegalovirus, the measles- and varicella-zoster viruses, and herpesvirus can also affect the lymph nodes. The characteristic viral inclusions are described elsewhere (see Chaps. 10 and 19).
Infectious mononucleosis is associated with EBV. It is a self-limited infectious disease that affects young patients and can result in fever, pharyngitis, rash, and cervical adenopathy. The axillary and inguinal lymph nodes can also be affected. Atypical lymphocytes are present in the peripheral blood. Most of these cases are diagnosed clinically and confirmed with a heterophil antibody (Monospot) test. However, some patients may have an unusual presentation of this disease, such as lymphadenopathy without associated symptoms, and their lymph nodes may have to be aspirated to confirm the diagnosis.
Aspirates of infectious mononucleosis can be quite variable, but they usually show a polymorphous population of small and large transformed lymphocytes, immunoblasts with binucleation, tingible body macrophages, plasma cells, eosinophils, and mast cells. The immunoblastic proliferation may be so florid that it may be mistaken for lymphoma, but the spectrum of immunoblastic maturation in cells with plasmacytoid features is not seen in lymphomas. Binucleated immunoblasts, resembling the Reed-Sternberg cells observed in Hodgkin lymphoma, have been described in infectious mononucleosis and postvaccinal lymphadenitis; however, these cells usually do not meet the strict criteria for Reed-Sternberg cells (Kardos et al, 1988; Stanley et al, 1990a).
Infection with Human Immunodeficiency Virus
Individuals infected with HIV commonly have lymphadenopathy. FNA is a useful tool to determine whether the enlarging lymph nodes are related to viral or opportunistic infections, Kaposi sarcoma, high-grade lymphoma, or metastatic carcinoma (Martin-Bates et al, 1990; Strigle et al, 1992). Needle aspiration biopsy and flow cytometry of lymph nodes has been proposed as potentially useful in assessing the clinical status of HIV-infected patients (Cajigas et al, 1997).
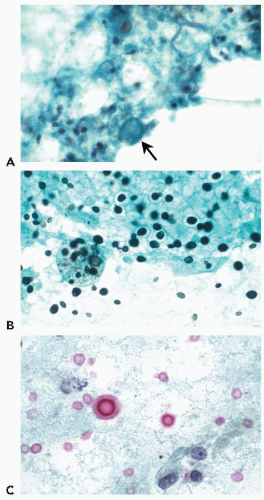
HIV lymphadenitis may be associated with a spectrum of changes, ranging from florid lymphoid hyperplasia to marked lymphoid depletion. As in other types of viral lymphadenitis, aspirates from florid lymphoid hyperplasia typically show a heterogeneous population of small, intermediate, and large lymphocytes; plasma cells; and tingible body macrophages (Oertel et al, 1990; Shabb et al, 1991). Multinucleated giant cells or polykaryocytes with multiple small nuclei that resemble osteoclasts (Warthin-Finkeldey cells, also seen in measles) and epithelioid histiocytes have also been observed. Oertel et al (1990) noted that lymph node aspirates from HIV-positive patients contained a higher number of immunoblasts than did those from HIV-negative patients. In some cases, the presence of numerous immature cells may be suggestive of lymphoma (Fig. 3-12). Immunophenotyping is usually helpful in confirming a polyclonal population.
In the depletion phase, aspirates often have sparse follicular center cells, immunoblasts, and tingible body macrophages but high numbers of plasma cells. Macrophages may also be seen. In such cases, infections caused by mycobacteria and fungi should be ruled out.
Granulomatous Lymphadenitis
In histologic sections, the presence of granulomas, composed of epithelioid and giant cells with or without central necrosis, is the hallmark of granulomatous lymphadenitis. Granulomas are approximately spherical structures of various sizes, composed of elongated epithelioid cells with pale, eosinophilic cytoplasm and giant cells, usually of Langhans type, with a garland of peripheral, small nuclei. Granulomatous lymphadenitis can be seen, not only in infectious processes such as tuberculosis, atypical mycobacteriosis, brucellosis, or infections caused by fungi or Pneumocystis carinii, but also in sarcoidosis, foreign-body reactions, non-Hodgkin lymphoma, Hodgkin lymphoma, and, rarely, lymph node-draining carcinoma.
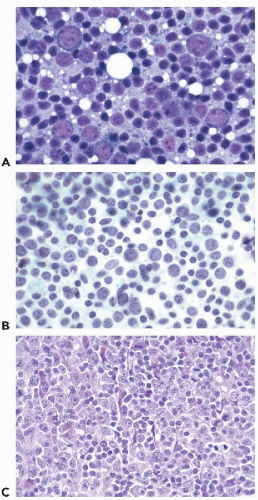
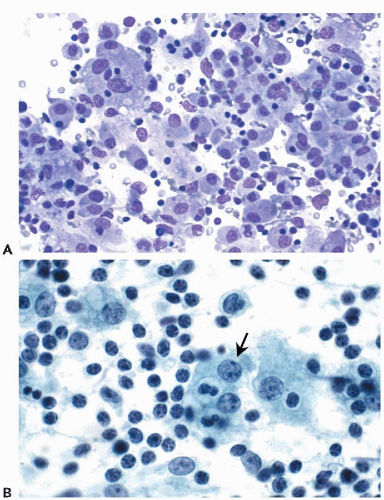
Figure 31-12 Reactive lymphoid hyperplasia.A,B. An increased number of transformed lymphocytes and paraimmunoblasts are present in this aspirate from a patient infected with human immunodeficiency virus. C. High magnification of the tissue section shows a spectrum of lymphoid cells including small lymphocytes, intermediate-size transformed cells, and immunoblasts. (A: Diff-Quik stain; B: Papanicolaou stain; A,B: oil immersion.)
Cytology
In aspirates, granulomatous lymphadenitis is characterized by epithelioid histiocytes in a background of lymphocytes and plasma cells. Epithelioid histiocytes are elongated polygonal cells with pale cytoplasm, indistinct cell borders, and elliptical, sometimes comma- or boomerang-shaped pale nuclei with finely granular chromatin, and frequently slight lateral indentations (Fig. 31-13). These cells may form loose aggregates or cohesive clusters that are reminiscent of granulomas when seen in tissue sections. Multinucleated giant cells of foreign-body-type with dispersed nuclei or Langhans type giant cells are often present. Granulomatous lymphadenitis may or may not show associated necrosis, which appears as acellular granular material on smears.
Figure 31-13 Granulomatous lymphadenitis.A. Epithelioid histiocytes and lymphocytes are seen in an aspirate from a patient with tuberculosis. B. Tissue section shows granulomas composed of epithelioid histiocytes and a Langhans-type giant cell.
Conditions Associated with Granulomatous Lymphadenitis
Mycobacterial infections, including those caused by Mycobacterium tuberculosis and atypical mycobacteria, are associated with granulomatous lymphadenitis. World-wide, tuberculosis is the leading infectious cause of morbidity and mortality. In the United States, the number of new cases of tuberculosis has increased over the last decade, primarily in areas where HIV infection is prevalent. Individuals at high risk for tuberculosis include infants and young children, elderly adults, and immunocompromised patients such as those infected with HIV.
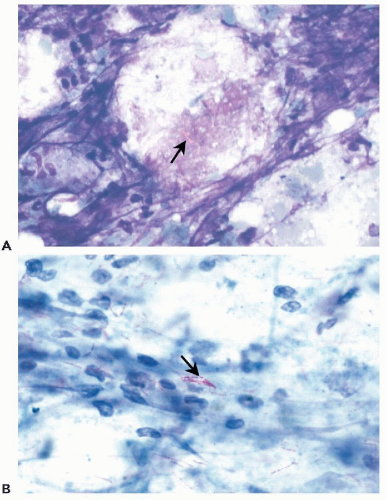
Very rarely, smears from the lymph nodes of patients with tuberculous lymphadenitis may show only necrotic material and neutrophils (Das, 2000). The presence of negative images of bacilli (Fig. 31-14) on air-dried Romanovsky’s stained smears is a helpful diagnostic clue that the lymph node is infected by mycobacteria (Stanley et al, 1990b; Ang et al, 1993). The acid-fast bacillus stain can be performed even on destained Papanicolaou-stained smears to identify mycobacterial organisms, although the detection rate is quite variable with this method.
Figure 31-14 Mycobacterial infection. A. Negative-images (arrow) of mycobacterial bacilli are seen in air-dried smears from a patient who had lymphadenopathy thought to be caused by lymphoma. B. Acid-fast stain shows long, beaded, filamentous bacilli (arrow) that were classified as Mycobacterium kansasii by culture. (A: Diff-Quik stain; B: Ziehl-Neelsen stain; A,B: oil immersion.)
Mycobacterium avium-intracellulareinfection should be considered when aggregates of large histiocytes are filled with negatively stained linear cytoplasmic inclusions, particularly in patients who are immunosuppressed (Shabb et al, 1991). In lepromatous leprosy, the characteristic cell is a syncytial histiocyte (Virchow or globus cell), which is frequently multinucleated and has a vacuolated cytoplasm that contains numerous lepra bacilli (Gupta et al, 1981).
Fungal infections, previously discussed in depth in Chapter 19, such as those caused by Histoplasma capsulatum, Coccidioides immitis, and Cryptococcus neoformans, may involve lymph nodes. Chaiwun et al (2002) reported eight HIV-positive patients with lymphadenopathy caused by Penicillium marneffei. The Gomori’s methenamine silver stain is helpful in detecting these organisms in cytologic preparations.
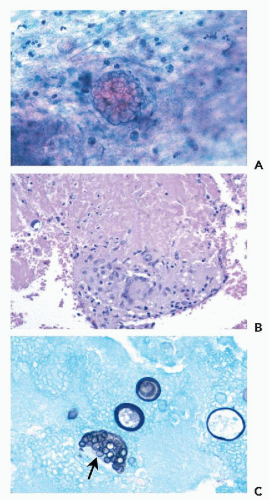
Histoplasmosis is endemic in the central part of the United States, while coccidioidomycosis is endemic in the southwestern regions. Histoplasmosis involving the mediastinal lymph nodes may be associated with inflammation and proliferation of fibrous tissue resulting in sclerosing mediastinitis. Aspirates of lymph nodes from patients with coccidioidomycosis often show extensive necrosis; careful examination may reveal thick-walled cysts containing endospores (Fig. 31-15). Cryptococcus may affect both immunocompetent and immunosuppressed patients. Aspirates of lymph nodes from infected patients show epithelioid histiocytes, yeast-filled giant cells, and lymphocytes (Fig. 31-16). The narrow-based budding yeasts usually have a thick mucopolysaccharide capsule that stains positive with mucicarmine stain. The Fontana-Masson stain, which provides the advantage of staining capsule-deficient organisms, can also be used (Ro et al, 1987).
Lymphadenitis in toxoplasmosis usually affects the posterior cervical lymph nodes, although other lymph nodes may be involved. Infection most commonly results from exposure to contaminated cat feces or ingestion of undercooked meat. Aspirates show a polymorphous lymphoid population admixed with loosely aggregated epithelioid histiocytes and tingible body macrophages. The crescent-shaped organisms are rarely observed in aspirates (Argyle et al, 1983). Pneumocystis carinii, discussed at length in Chapter 19, can also cause granulomatous lymphadenitis in AIDS.
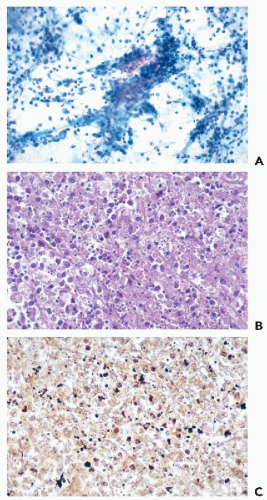
Figure 31-15Coccidiomycosis immitis.A. Smear shows a spherule in a background of acute inflammatory cells. B. Cell block shows an aggregate of lymphocytes, epithelioid histiocytes, and a multinucleated giant cell in a background of necrosis. C. A mature spherule contains endospores (arrow). (A: High magnification; B: H & E stain; C: Gomori’s methenamine silver stain, high magnification.)
Figure 31-16 Cryptococcal lymphadenitis.A. Smear shows histiocytes (arrow) with phagocytized material. B. Gomori methenamine silver stain shows yeast (arrow) varying in size with occasional narrow-based budding. C. A mucicarmine stain highlights the thick mucopolysaccharide capsule. (A-C: Oil immersion.)
Lymphadenitis associated with rhinoscleroma was reported by Gera et al (1995). Large macrophages, known as Mikulicz cells, containing Gram-negative bacteria, were observed.
Sarcoidosis is a granulomatous disease of unknown cause that affects blacks more frequently than whites. The disease is usually diagnosed in the third and fourth decades of life. It can affect any organ, including cervical and hilar lymph nodes (Frable and Frable, 1984; Morales et al, 1994). For a discussion of the cytologic presentation of sarcoidosis, see Chapter 19. Similar granulomas may occur in lymph nodes draining metastatic cancer.
Cat-scratch disease is caused by a pleomorphic Gramnegative bacillus, Bartonella henselae. The disease should be suspected if the aspirate from an axillary or neck lymph node reveals granulomatous inflammation accompanied by neutrophils, necrosis, and occasional multinucleated giant cells (suppurative granulomatous inflammation) (Fig. 31-17) in a young patient who has had close contact with a cat.
Figure 31-17 Suppurative granulomatous inflammation.A. Inflammatory cells are admixed with epithelioid histiocytes in this aspirate from a patient whose clinical history was consistent with cat-scratch disease.B. Tissue sections show neutrophils, histiocytes, and extensive necrosis. C. Small aggregates of bacteria are visible on the Warthin-Starry stain. (B,C: high magnification.)
Lymphogranuloma venereum, caused by Chlamydia trachomatis, should be considered when the aspirate of an inguinal lymph node exhibits suppurative granulomatous inflammation (see Chap. 10). Similar findings may be observed in the rare tularemia (caused by Francisella tularensis, transmitted from rabbits and other rodents) and in the abdominal lymph nodes in the equally rare intestinal infection by the Gram-negative organism Yersinia(enterocolicaorpseudotuberculosis).
Sinusoidal Expansion Of Lymph Nodes
Sinus histiocytosis is a common type of lymph node hyperplasia that affects mainly the axillary and inguinal areas. This type of hyperplasia may also be observed in lymph nodes that drain cancers. In histologic sections of lymph nodes, the markedly dilated sinuses are filled with macrophages that have abundant, foamy cytoplasm. In aspirates, a few macrophages with phagocytic material and occasional neutrophils are seen.
Conditions Associated with Sinusoidal Expansion
Sinus histiocytosis with massive lymphadenopathy, also known as Rosai-Dorfman disease, is a benign, generally self-limited condition. It usually affects children and adolescents, occurs more frequently in black than white patients, and is characterized by bilateral cervical lymphadenopathy, leukocytosis, and an elevated erythrocyte sedimentation rate. Aspirates usually contain numerous histiocytes, some containing whole lymphocytes within their cytoplasm (a phenomenon known as emperipolesis) (Fig. 31-18), plasma cells, and few neutrophils (Pettinato et al, 1990; Deshpande et al, 2000).
Langerhans cell histiocytosis is a rare disorder, usually occurring in children and young adults. It most commonly presents as a single lytic bone lesion (eosinophilic granuloma), composed of mature, lipid-laden histiocytes, Langerhans’ cells with pale eosinophilic cytoplasm, and a finely textured characteristically indented or grooved nuclei and varying numbers of eosinophils, plasma cells, and neutrophils with a few multinucleated giant cells. Less commonly, Langerhans-cell histiocytosis is multifocal and may involve soft tissue including lymph nodes, sometimes with the triad of Hand Schuller Christian disease (exophthalmos, diabetes insipidus, and bone defects). Langerhans cells are dendritic cells, normally present in the epidermis and other epithelia, and are thought to play a role in the immunologic response of the skin. They are antigen-presenting cells characterized by expression of CD-1a antigen and the presence of tennis racquet-shaped tubular cytoplasmic structures (Birbeck granules) on ultrastructural examination. In needle aspirates, the Langerhans cells have a striking similarity to the macrophages observed in sinus histiocytosis, except for their convoluted and grooved nuclei and the absence of phagocytosis (Koss et al, 1992). Their identity can be confirmed by staining with CD-1a antibody. Needle aspiration smears usually also contain eosinophils and multinucleated giant cells, plasma cells, and neutrophils; the presence of eosinophils should always alert one to this diagnosis (Pohar-Marinsek and Us-Krasovec, 1996; Kakkar et al, 2001).
Figure 31-18 Sinus histiocytosis with massive lymphadenopathy.A. Numerous histiocytes (macrophages) are present. B. Note the histiocyte (macrophage) with emperipolesis (arrow). (A: Diff-Quik stain, high magnification; B: Papanicolaou stain, oil immersion.)
Phagocytosis of foreign material may be associated with lymphadenopathy. In the past, lymphangiography was performed to visualize retroperitoneal lymph nodes in suspected lymphoma or metastatic carcinoma. A radio-opaque oily material, injected into the lymphatics of the dorsum of the foot, is transported to retroperitoneal lymph nodes and phagocytized by macrophages. Aspiration of such lymph nodes results in the so-called lymphangiogram effect. The smears show large, lipid-laden histiocytes, multinucleated giant cells, and eosinophils. Leaking or rupture of silicone implants used in breast augmentations or joint prostheses may result in silicone reaching the regional lymph nodes, which are generally enlarged. Aspirates from the lymph nodes of such patients may show silicone lymphadenopathy, which is characterized by the presence of numerous vacuolated macrophages and multinucleated giant cells. The vacuoles contain silicon, a refractile homogeneous material that is not birefringent. Asteroid bodies, which are crystalloid structures resembling stars, may be seen in the cytoplasm of the macrophages (Tabatowski et al, 1990; Dodd et al, 1993). It is of interest that asteroid bodies may also be observed in sarcoidosis (see Chap. 19).
POSTTRANSPLANTATION LYMPHOPROLIFERATIVE DISORDERS
Posttransplantation lymphoproliferative disorders occur in approximately 2% of organ-transplant recipients who were given immunosuppressive therapy. Epstein-Barr virus (EBV) is commonly associated with these disorders. Their recognition is important because, unlike conventional lymphomas, they may respond to a decrease in the dosage of immunosuppressive treatments, whereas continued immunosuppression may lead to disease progression. Further, these disorders may not respond to conventional chemotherapy (Knowles et al, 1995).
Aspirates from patients who have posttransplantation lymphoproliferative disorder may have either a polymorphous or monomorphous cell population. In the former, aspirates show a heterogeneous population of mature and immature lymphocytes, with scattered plasma cells and histiocytes in the background, whereas aspirates from the latter contain predominantly large cells resembling lymphoma (Gattuso et al, 1997; Dusenbery et al, 1997).
Knowles et al (1995) classified posttransplantation lymphoproliferative disorders into three categories according to distinct morphologic and molecular findings:
Plasmacytic hyperplasia
Polymorphic B-cell hyperplasia and polymorphic B-cell lymphoma
Immunoblastic lymphoma or multiple myeloma
In plasmacytic hyperplasia, the cells are usually polyclonal, contain multiple forms of EBV, and lack oncogene and tumor suppressor gene alterations. In polymorphic B-cell hyperplasia and polymorphic B-cell lymphoma, cells are usually monoclonal, contain a single form of EBV, and lack oncogene and tumor suppressor gene alterations. The patients with immunoblastic lymphoma or multiple myeloma have widespread disease and the cells are monoclonal, contain a single form of EBV, and have alterations of one or more oncogenes or tumor suppressor genes. For further discussion of these entities, see below.
Many of the limitations of FNA in the diagnosis of lymphoproliferative disorders have been addressed by Katz and Caraway (1995). One of the major drawbacks to the use of FNA is the lack of lymph node architecture that is important in the subclassification of some lymphomas. However, because many lymphomas have distinctive cytomorphologic, immunophenotypic, and proliferative profiles, the absence of architecture can be overcome in these instances by immunophenotyping. A subsequent lymph node excision should always be performed if the material is inadequate, if the results are ambiguous, or if the clinical and radiographic findings are not in accord with the cytologic interpretation.
Classification of Lymphomas
Over the last 50 years, several systems have been proposed to classify malignant lymphomas. New systems have been formulated as the sequence of events in the turnover and maturation of lymphocytes has become better understood. Three discoveries were especially important in this process: the first was the observation that the basic characteristics of normal B and T lymphocytes may be retained by the lymphoma cells; the second was the recognition that small lymphocytes are a resting form of the cell that can undergo a series of notable metamorphoses, leading to the formation of large, metabolically active cells; and the third was the recognition that non-Hodgkin lymphomas exhibit both diffuse and nodular or follicular forms. In the latter form, the tumor tends to mimic the formation of lymphoid follicles and, sometimes, their germinal centers.
Early classification systems used primarily tissue architecture, the cytologic features of the cells, or both. In the 1980s, the complexity of the Rappaport (1966), Lukes and Collins (1974), and Lennert from Kiel (1967) classification systems prompted the U.S. National Cancer Institute to classify non-Hodgkin lymphomas into groupings with some prognostic value (Koss et al, 1992). The resulting classification, known as the Working Formulation (non-Hodgkin pathologic project, 1982) of non-Hodgkin lymphomas had three grades: low, intermediate, and high, all three derived strictly from morphologic appearance. Since then, remarkable progress has been made in our understanding of lymphomas on the basis of laboratory findings such as morphologic features, immunophenotype, cytogenetic features, molecular analysis, and clinical manifestations and course of the disease (Jaffe et al, 1999). The information from these findings has been used to develop the Revised European-American Classification of Lymphoid Neoplasms (REAL), proposed by the International Lymphoma Study Group (Harris et al, 1994). The REAL system categorizes entities on the basis of the neoplasm’s cell of origin. Because this system places greater emphasis than previous systems on cytomorphologic features, immunophenotype, and results of molecular studies, it can be applied easily, using a multiparameter approach to FNA specimens. The new (1998) World Health Organization (WHO) classification for lymphomas (Table 31-3) is similar to the REAL system; minor modifications have been made as additional data have become available (Jaffe et al, 1999).
TABLE 31-3 WORLD HEALTH ORGANIZATION CLASSIFICATION OF THE NEOPLASTIC DISEASES OF THE LYMPHOID TISSUES
This chapter highlights the B-cell lymphomas, which are the most common in everyday practice. T-cell lymphomas are briefly discussed but not all the lymphomas listed in the REAL or updated WHO classifications are discussed.
Principles of Cytologic Diagnosis of Malignant Lymphomas
The population of cells in non-Hodgkin’s lymphomas is usually monotonous, that is, the cells are of approximately equal sizes. There are some exceptions to this rule, described below. Cells of malignant lymphomas in well-prepared smears appear singly and do not form clusters. In poorly prepared smears, overlapping of cells may sometimes be observed. In assessing smears, the lymphoid cells are classified as “small” if they are equal in size or slightly larger than normal resting lymphocytes; “intermediate” if they are one and one-half times larger than the size of a normal lymphocyte but not larger than the nucleus of a macrophage; or “large” if they are two or more times the size of a normal lymphocyte.
The nuclei may be round, cleaved, or lobulated, or show irregularities of the membrane with small protrusions. The coarse or fine patterns of chromatin distribution and the presence or absence of nucleoli must be noted.
Lymphoglandular bodies (Søderstrøm bodies) discussed in the opening pages of this chapter, are helpful in recognizing the lymphocytic origin of a neoplasm if the cell population is difficult to classify, as is sometimes the case in large-cell lymphomas. Although Bangerter et al (1997) considered the Søderstrøm bodies to be specific for malignant lymphomas and related disorders, they are commonly observed in benign aspirates and, rarely, in other malignancies as well.
B-Cell Lymphoma
Mature B-cell lymphomas comprise the majority of lymphoid neoplasms worldwide and are more common in developing countries. The subclassification of these neoplasms requires a multiparameter approach.
Small Lymphocytic Lymphoma
Most cases of the small lymphocytic lymphomas occur in older adults, and most patients have bone marrow and peripheral blood involvement, although occasionally the disease is limited to the lymph nodes. Many patients with the latter form eventually develop disease in the bone marrow and blood. The clinical course is indolent but the disease is not curable. The disease may undergo transformation into prolymphocytic lymphoma, large-cell lymphoma (Richter syndrome), or, rarely, Hodgkin lymphoma.
Cytology
Small lymphocytic lymphoma comprises a monomorphous population of small, round lymphocytes with nuclei that have a checkerboard pattern of clumped chromatin, known as “cellules grumelées” (Fig. 31-19). For a detailed discussion of these cells see Chapters 26 and 27. Scattered in the background are large cells—prolymphocytes and paraimmunoblasts. Prolymphocytes are slightly larger than paraimmunoblasts, but both have round nuclei with prominent nucleoli and gray-blue cytoplasm.
An increase in the numbers of paraimmunoblasts (Fig. 31-20) may indicate a more aggressive clinical course than that of typical small lymphocytic lymphoma (Pugh et al, 1988).
Other cytologic manifestations of unfavorable accelerated course are plasmacytoid cells, mitotic figures, apoptotic bodies, necrosis, and a myxoid, dirty background (Shin et al, 2003). The predominance of large cells is indicative of a transformation of small cell lymphoma into a large B-cell lymphoma (Richter lymphoma).
Ancillary Studies
Immunophenotyping demonstrates a light chain restriction to either kappa or lambda expression (Fig. 31-21) and positivity for B-cell-associated antigens (CD19 and CD20), CD5, CD43, and CD23, but negativity for CD10 and FMC7. DNA ploidy analysis of small lymphocytic lymphoma shows a diploid population with low proliferative activity (mean Ki-67 labeling index of 5%) (Katz, 1993c), whereas transformed large-cell lymphomas have high proliferative activity.
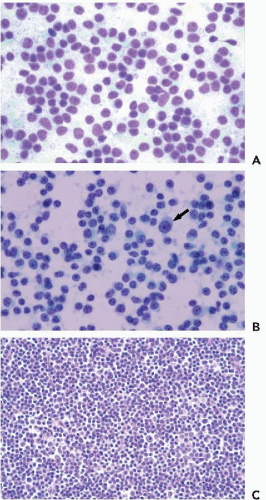
Figure 31-19 Small lymphocytic lymphoma.A,B. Aspirate is composed predominantly of small round cells with clumped chromatin and rare paraimmunoblasts (arrow). C. Tissue section shows a diffuse infiltrate of small lymphocytes with occasional paraimmunoblasts. (A: Diff-Quik stain; B: Papanicolaou stains.)
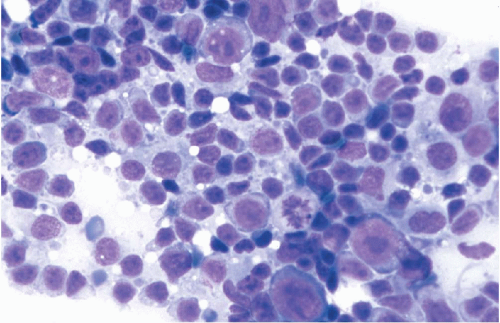
Figure 31-20 Small lymphocytic lymphoma with increased paraimmunoblasts. The increased number of paraimmunoblasts and presence of mitotic figures are suggestive of an accelerated phase of small lymphocytic lymphoma. (Diff-Quik stain.)
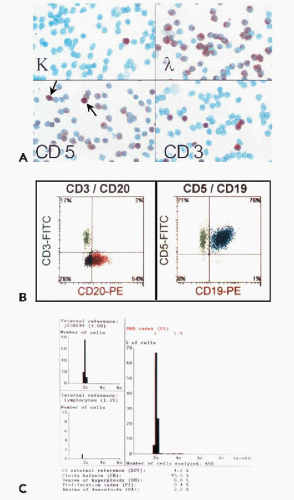
Figure 31-21 Small cell lymphocytic lymphoma.A. Immunocytochemical studies show monoclonal staining for lambda and CD5 positivity. Note that the CD5 staining is fainter in the B cells than in the T cells (arrows). B. Flow cytometry shows T-cell (CD3+) and B-cell (CD20+) population. There are also cells with CD19 and CD5 coexpression. C. DNA ploidy by image analysis reveals a diploid cell population and no proliferation index indicative of a low-grade lymphoma. (A: Immunoperoxidase stain.)
Trisomy 12 is present in one-third of small lymphocytic lymphoma (Knuutila et al, 1986). It may be demonstrated by FISH on cytospin aspirations with a centromeric probe (Caraway et al, 2000). Deletion of chromosome 13q14 is more common than trisomy 12 (Najfeld, 2003). Immunoglobulin heavy and light chain genes are rearranged (Harris et al, 1994).
Differential Diagnosis
Although both small lymphocytic lymphoma and mantle cell lymphoma show aberrant coexpression of CD5 and CD19 and lack CD10, small lymphocytic lymphoma is positive for CD23, whereas mantle cell lymphoma is not. Both follicular lymphoma and marginal zone lymphoma are CD5 negative. Lymphocyte-predominant Hodgkin lymphoma should be considered if pale polyploid cells with prominent nucleoli (so-called lymphohistiocytic, L&H, or “popcorn” cells) appear in a background of mature lymphocytes instead of paraimmunoblasts.
Lymphoplasmacytic Lymphoma
Lymphoplasmacytic lymphoma occurs primarily in older adults and can involve the bone marrow, lymph nodes, and spleen; peripheral blood and extranodal sites are less frequently affected. Most patients have an elevated level of monoclonal serum paraprotein of the immunoglobulin M type that sometimes results in symptoms of hyperviscosity (Waldenström macroglobulinemia).
Only gold members can continue reading. Log In or Register to continue