6
Lower Limb
Deep fascia and the saphenous opening
Tarsal tunnel, retinacula, and arrangement of major structures at the ankle
ADDITIONAL LEARNING RESOURCES FOR CHAPTER 6, LOWER LIMB, ON STUDENT CONSULT (www.studentconsult.com):
 Image Library — illustrations of lower limb anatomy, Chapter 6
Image Library — illustrations of lower limb anatomy, Chapter 6
 Self-Assessment (scored) — National Board style multiple-choice questions, Chapter 6
Self-Assessment (scored) — National Board style multiple-choice questions, Chapter 6
 Short Questions (not scored) — National Board style multiple-choice questions, Chapter 6
Short Questions (not scored) — National Board style multiple-choice questions, Chapter 6
 Interactive Surface Anatomy — interactive surface animations, Chapter 6
Interactive Surface Anatomy — interactive surface animations, Chapter 6
 PT Case Studies
PT Case StudiesAchilles tendinitis and tendinosis
See more PT Case Studies online
 Medical Clinical Case Studies
Medical Clinical Case Studies Clinical Cases
Clinical Cases
Regional anatomy
The lower limb is divided into the gluteal region, thigh, leg, and foot on the basis of major joints, component bones, and superficial landmarks (Figs. 6.1, 6.2):
 The gluteal region is posterolateral and between the iliac crest and the fold of skin (gluteal fold) that defines the lower limit of the buttocks. The major bone of the gluteal region is the pelvic bone.
The gluteal region is posterolateral and between the iliac crest and the fold of skin (gluteal fold) that defines the lower limit of the buttocks. The major bone of the gluteal region is the pelvic bone. Anteriorly, the thigh is between the inguinal ligament and the knee joint—the hip joint is just inferior to the middle third of the inguinal ligament, and the posterior thigh is between the gluteal fold and the knee. The bone of the thigh is the femur.
Anteriorly, the thigh is between the inguinal ligament and the knee joint—the hip joint is just inferior to the middle third of the inguinal ligament, and the posterior thigh is between the gluteal fold and the knee. The bone of the thigh is the femur. The leg is between the knee and ankle joints. The bones of the leg are the tibia and fibula.
The leg is between the knee and ankle joints. The bones of the leg are the tibia and fibula.
 The foot is distal to the ankle joint. Bones of the foot are the tarsals, metatarsals, and phalanges.
The foot is distal to the ankle joint. Bones of the foot are the tarsals, metatarsals, and phalanges.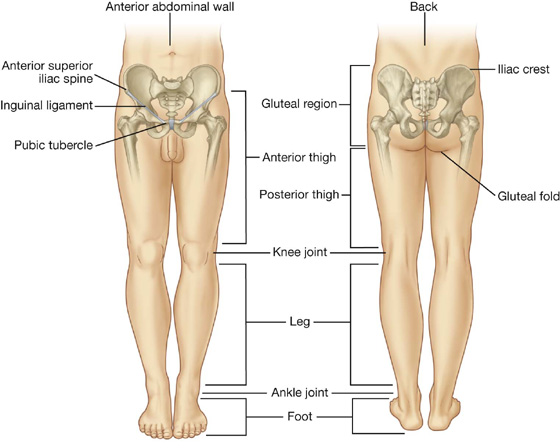
Fig. 6.1 Regions of the lower limb.
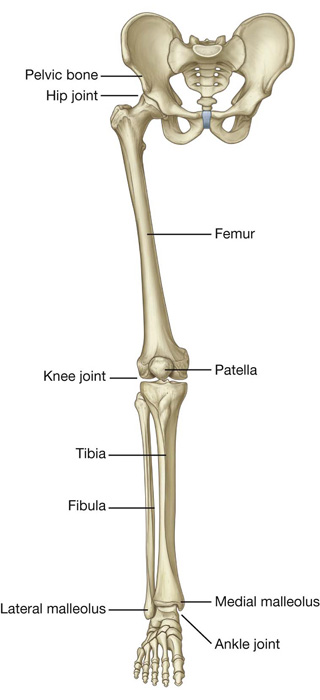
Fig. 6.2 Bones and joints of the lower limb.
The major functions of the lower limb are:
 to support the weight of the body when standing, and
to support the weight of the body when standing, and
 to move the body through space.
to move the body through space.
When standing erect, the line of the center of gravity is slightly posterior to the hip joints, anterior to the knee and ankle joints, and directly over the almost circular support base formed by the feet on the ground. The organization of ligaments at the hip and knee joints, together with the shape of the articular surfaces, particularly at the knee, facilitates “locking” of these joints into position, thereby reducing the muscular energy required to maintain a standing position.
When walking, integration of movements at all joints in the lower limb positions the foot on the ground and moves the body smoothly over the foot with minimal changes in the position of the body’s center of gravity.
The lower limb is directly anchored to the axial skeleton by a sacroiliac joint and by strong ligaments, which link the pelvic bone to the sacrum. This design serves to transmit the weight of the body above to the lower limb below.
Movements at the hip joint are flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction (Fig. 6.3).
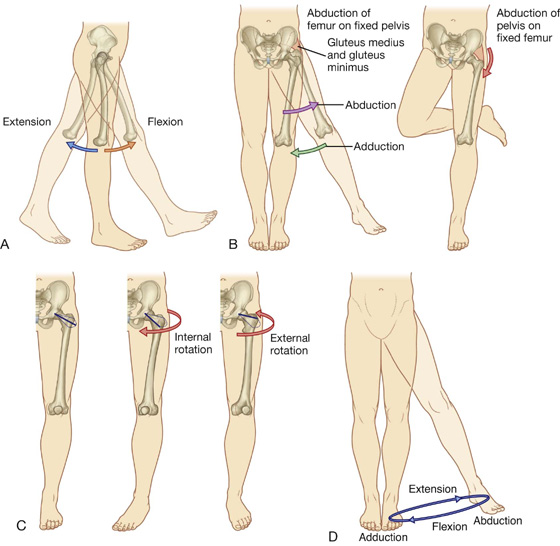
Fig. 6.3 Movements of the hip joint. A. Flexion and extension. B. Abduction and adduction. C. External and internal rotation. D. Circumduction.
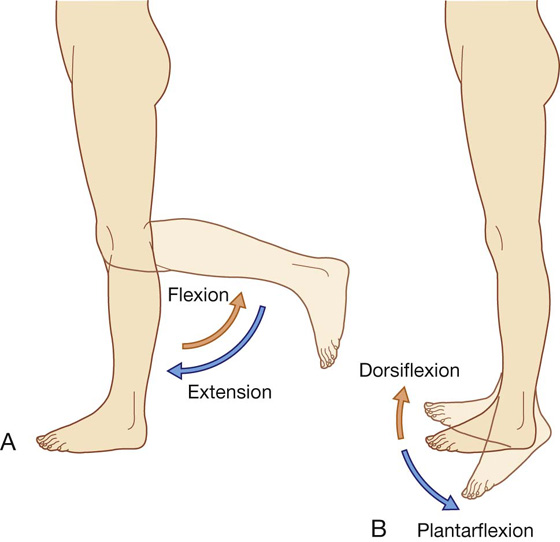
The knee and ankle joints are primarily hinge joints. Movements at the knee are mainly flexion and extension (Fig. 6.4A). Movements at the ankle are dorsiflexion (movement of the dorsal side of foot toward the leg) and plantarflexion (Fig. 6.4B).
THE HIP
Bony pelvis
The external surfaces of the pelvic bones, sacrum, and coccyx are predominantly the regions of the pelvis associated with the lower limb, although some muscles do originate from the deep or internal surfaces of these bones and from the deep surfaces of the lumbar vertebrae, above.
Each pelvic bone is formed by three bones (ilium, ischium, and pubis), which fuse during childhood. The ilium is superior and the pubis and ischium are anteroinferior and posteroinferior, respectively (Fig. 6.5).
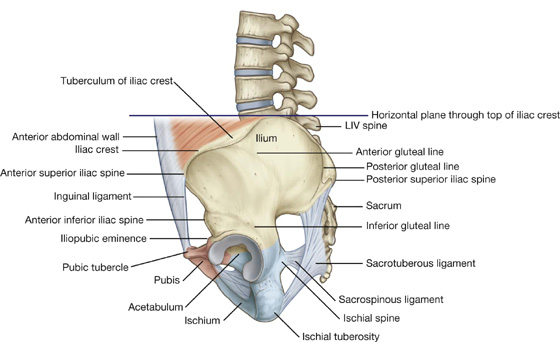
Fig. 6.5 External surface of the bony pelvis. Lateral view.
Ilium
The upper fan-shaped part of the ilium is associated on its inner side with the abdomen and on its outer side with the lower limb. The top of this region is the iliac crest, which ends anteriorly as the anterior superior iliac spine and posteriorly as the posterior superior iliac spine (Fig. 6.5). A prominent lateral expansion of the crest just posterior to the anterior superior iliac spine is the tuberculum of iliac crest.
The anterior inferior iliac spine is on the anterior margin of the ilium, and below this, where the ilium fuses with the pubis, is a raised area of bone (the iliopubic eminence [Fig. 6.5]).
The gluteal surface of the ilium faces posterolaterally, lies below the iliac crest, and provides attachment for the gluteal muscles. It is marked by three curved lines (inferior, anterior, and posterior gluteal lines (Fig. 6.5):
 The inferior gluteal line originates just superior to the anterior inferior iliac spine and curves inferiorly across the bone to end near the posterior margin of the acetabulum.
The inferior gluteal line originates just superior to the anterior inferior iliac spine and curves inferiorly across the bone to end near the posterior margin of the acetabulum. The anterior gluteal line originates from the lateral margin of the iliac crest between the anterior superior iliac spine and the tuberculum of iliac crest, and arches inferiorly across the ilium to disappear just superior to the upper margin of the greater sciatic foramen.
The anterior gluteal line originates from the lateral margin of the iliac crest between the anterior superior iliac spine and the tuberculum of iliac crest, and arches inferiorly across the ilium to disappear just superior to the upper margin of the greater sciatic foramen. The posterior gluteal line descends almost vertically from the iliac crest to a position near the posterior inferior iliac spine.
The posterior gluteal line descends almost vertically from the iliac crest to a position near the posterior inferior iliac spine.Ischial tuberosity
The ischial tuberosity is posteroinferior to the acetabulum and is associated mainly with the hamstring muscles of the posterior thigh (Fig. 6.6). It is divided into upper and lower areas by a transverse line.
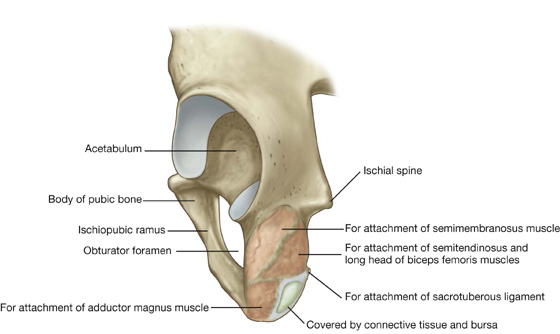
Fig. 6.6 Ischial tuberosity. Posterolateral view.
The upper area of the ischial tuberosity is oriented vertically and is further subdivided into two parts by an oblique line, which descends, from medial to lateral, across the surface.
The lower area of the ischial tuberosity is oriented horizontally and is divided into medial and lateral regions by a ridge of bone.
When sitting, this medial part supports the body weight.
The sacrotuberous ligament is attached to a sharp ridge on the medial margin of the ischial tuberosity.
Ischiopubic ramus and pubic bone
The external surfaces of the ischiopubic ramus anterior to the ischial tuberosity and the body of the pubis provide attachment for muscles of the medial compartment of the thigh (Fig. 6.6).
Acetabulum
The large cup-shaped acetabulum for articulation with the head of the femur is on the lateral surface of the pelvic bone in the region where the ilium, pubis, and ischium fuse (Fig. 6.7).
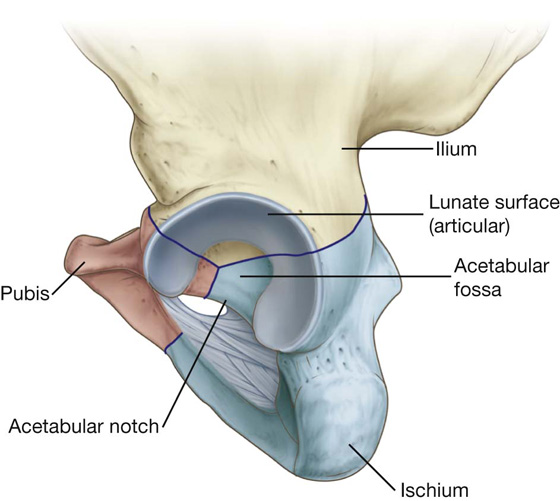
Fig. 6.7 Acetabulum.
The margin of the acetabulum is marked inferiorly by a prominent notch (acetabular notch).
The wall of the acetabulum consists of nonarticular and articular parts:
 The nonarticular part is rough and forms a shallow circular depression (the acetabular fossa) in central and inferior parts of the acetabular floor; the acetabular notch is continuous with the acetabular fossa (Fig. 6.7).
The nonarticular part is rough and forms a shallow circular depression (the acetabular fossa) in central and inferior parts of the acetabular floor; the acetabular notch is continuous with the acetabular fossa (Fig. 6.7).
 The articular (lunate) surface is broad and surrounds the anterior, superior, and posterior margins of the acetabular fossa (Fig. 6.7).
The articular (lunate) surface is broad and surrounds the anterior, superior, and posterior margins of the acetabular fossa (Fig. 6.7).
The smooth crescent-shaped articular surface (the lunate surface) is broadest superiorly where most of the body’s weight is transmitted through the pelvis to the femur. The lunate surface is deficient inferiorly at the acetabular notch (Fig. 6.7).
The acetabular fossa provides attachment for the ligament of the head of the femur, whereas blood vessels and nerves pass through the acetabular notch.
Clinical app
Pelvic fractures
There are many ways of classifying pelvic fractures, which enable a surgeon to determine the appropriate treatment and the patient’s prognosis. The pelvic bones, sacrum, and associated joints form a bony ring surrounding the pelvic cavity.
Pelvic fractures are generally of four types.
 Type 1 injuries occur without disruption of the bony pelvic ring (e.g., a fracture of the iliac crest). These types of injuries are unlikely to represent significant trauma, though in the case of a fracture of the iliac crest, blood loss needs to be assessed.
Type 1 injuries occur without disruption of the bony pelvic ring (e.g., a fracture of the iliac crest). These types of injuries are unlikely to represent significant trauma, though in the case of a fracture of the iliac crest, blood loss needs to be assessed. Type 2 injuries occur with a single break in the bony pelvic ring. An example of this would be a single fracture with diastasis (separation) of the pubic symphysis.
Type 2 injuries occur with a single break in the bony pelvic ring. An example of this would be a single fracture with diastasis (separation) of the pubic symphysis. Type 3 injuries occur with double breaks in the bony pelvic ring. These include bilateral fractures of the pubic rami, which may produce urethral damage.
Type 3 injuries occur with double breaks in the bony pelvic ring. These include bilateral fractures of the pubic rami, which may produce urethral damage. Type 4 injuries occur at and around the acetabulum.
Type 4 injuries occur at and around the acetabulum.
Other types of pelvic ring injuries include disruption of the sacroiliac joint with or without dislocation. This may involve significant visceral pelvic trauma and hemorrhage.
Other general pelvic injuries include stress fractures and insufficiency fractures, as seen in athletes and in elderly patients with osteoporosis, respectively.
Proximal femur
The femur is the bone of the thigh and the longest bone in the body. Its proximal end is characterized by a head and neck, and two large projections (the greater and lesser trochanters) on the upper part of the shaft (Fig. 6.8).
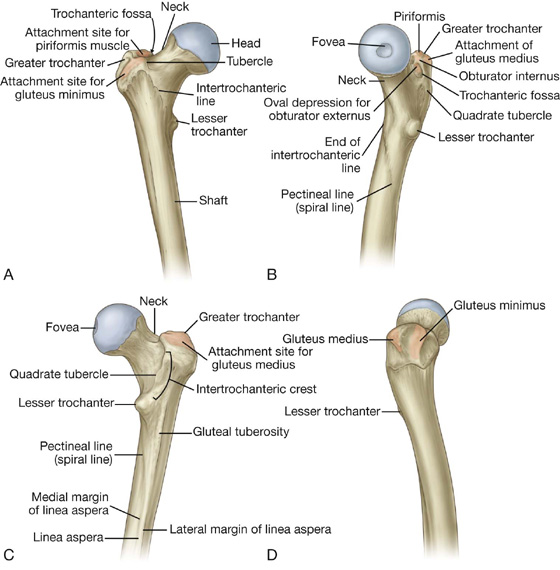
The head of the femur is spherical and articulates with the acetabulum of the pelvic bone. It is characterized by a nonarticular pit (fovea) on its medial surface for the attachment of the ligament of the head.
The neck of the femur is a cylindrical strut of bone that connects the head to the shaft of the femur. It projects superomedially from the shaft at an angle of approximately 125°, and projects slightly forward. The orientation of the neck relative to the shaft increases the range of movement of the hip joint.
The upper part of the shaft of the femur bears a greater and lesser trochanter, which are attachment sites for muscles that move the hip joint.
Greater and lesser trochanters
The greater trochanter extends superiorly from the shaft of the femur just lateral to the region where the shaft joins the neck of the femur (Fig. 6.8). It continues posteriorly where its medial surface is deeply grooved to form the trochanteric fossa. The lateral wall of this fossa bears a distinct oval depression for attachment of the obturator externus muscle.
The greater trochanter has an elongate ridge on its anterolateral surface for attachment of the gluteus minimus and a similar ridge more posteriorly on its lateral surface for attachment of the gluteus medius. Between these two points, the greater trochanter is palpable.
On the medial side of the superior aspect of the greater trochanter and just above the trochanteric fossa is a small impression for attachment of the obturator internus and its associated gemelli muscles, and immediately above and behind this feature is an impression on the margin of the trochanter for attachment of the piriformis muscle.
The lesser trochanter is smaller than the greater trochanter and has a blunt conical shape. It projects posteromedially from the shaft of femur just inferior to the junction with the neck (Fig. 6.8). It is the attachment site for the combined tendons of psoas major and iliacus muscles.
Extending between the two trochanters and separating the shaft from the neck of the femur are the intertrochanteric line and intertrochanteric crest.
Intertrochanteric line
The intertrochanteric line is a ridge of bone on the anterior surface of the upper margin of the shaft that descends medially from a tubercle on the anterior surface of the base of the greater trochanter to a position just anterior to the base of the lesser trochanter (Fig. 6.8). It is continuous with the pectineal line (spiral line), which curves medially under the lesser trochanter and around the shaft of the femur to merge with the medial margin of the linea aspera on the posterior aspect of the femur.
Intertrochanteric crest
The intertrochanteric crest is on the posterior surface of the femur and descends medially across the bone from the posterior margin of the greater trochanter to the base of the lesser trochanter (Fig. 6.8). It is a broad smooth ridge of bone with a prominent tubercle (the quadrate tubercle) on its upper half, which provides attachment for the quadratus femoris muscle.
Shaft of the femur
The shaft of the femur descends from lateral to medial in the coronal plane at an angle of 7° from the vertical axis (Fig. 6.9). The distal end of the femur is therefore closer to the midline than the upper end of the shaft.
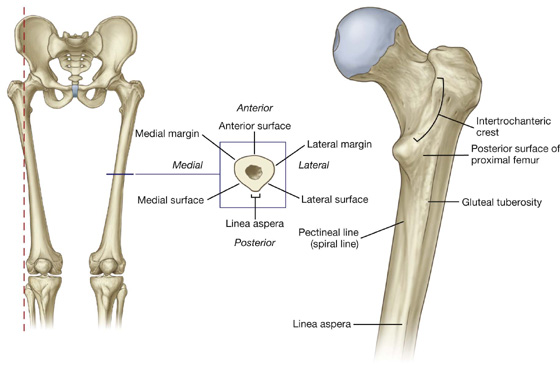
Fig. 6.9 Shaft of the femur. On the right is a posterior view of proximal shaft of right femur.
The middle third of the shaft of the femur is triangular in shape with smooth lateral and medial margins between anterior, lateral (posterolateral), and medial (posteromedial) surfaces. The posterior margin is broad and forms a prominent raised crest (the linea aspera) (Fig. 6.9).
The linea aspera is a major site of muscle attachment in the thigh. In the proximal third of the femur, the medial and lateral margins of the linea aspera diverge and continue superiorly as the pectineal line and gluteal tuberosity, respectively (Fig. 6.9):
 The pectineal line curves anteriorly under the lesser trochanter and joins the intertrochanteric line.
The pectineal line curves anteriorly under the lesser trochanter and joins the intertrochanteric line. The gluteal tuberosity is a broad linear roughening that curves laterally to the base of the greater trochanter.
The gluteal tuberosity is a broad linear roughening that curves laterally to the base of the greater trochanter.The gluteus maximus muscle is attached to the gluteal tuberosity.
The triangular area enclosed by the pectineal line, the gluteal tuberosity, and the intertrochanteric crest is the posterior surface of the proximal end of the femur (Fig. 6.9).
Clinical app
Femoral neck fractures
Femoral neck fractures (Fig. 6.10) can interrupt blood supply to the femoral head. Blood supply to the head and neck is primarily from an arterial ring formed around the base of the femoral neck. From here, vessels course along the neck, penetrate the capsule, and supply the femoral head. Blood supply to the femoral head and femoral neck is further enhanced by the artery of the ligamentum teres, which is generally small and variable. Femoral neck fractures may disrupt associated vessels and lead to necrosis of the femoral head.

Clinical app
Intertrochanteric fractures
In these fractures, the break usually runs from the greater trochanter through to the lesser trochanter and does not involve the femoral neck. Intertrochanteric fractures preserve the femoral neck blood supply and do not render the femoral head ischemic.
Clinical app
Femoral shaft fractures
An appreciable amount of energy is needed to fracture the femoral shaft. This type of injury is therefore accompanied by damage to the surrounding soft tissues, which include the muscle compartments and the structures they contain.
Hip joint
The hip joint is a synovial articulation between the head of the femur and the acetabulum of the pelvic bone (Fig. 6.11A; also see Fig. 6.16). The joint is a multiaxial ball and socket joint designed for stability and weightbearing at the expense of mobility.
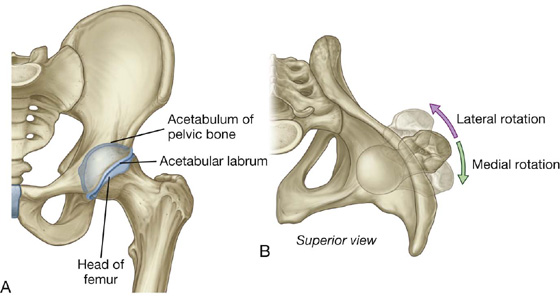
When considering the effects of muscle action on the hip joint, the long neck of the femur and the angulation of the neck on the shaft of the femur must be kept in mind. For example, medial and lateral rotation of the femur involves muscles that move the greater trochanter forward and backward, respectively, relative to the acetabulum (Fig. 6.11B).
The articular surfaces of the hip joint are:
 the spherical head of the femur, and
the spherical head of the femur, and
 the lunate surface of the acetabulum of the pelvic bone (Fig. 6.12A).
the lunate surface of the acetabulum of the pelvic bone (Fig. 6.12A).
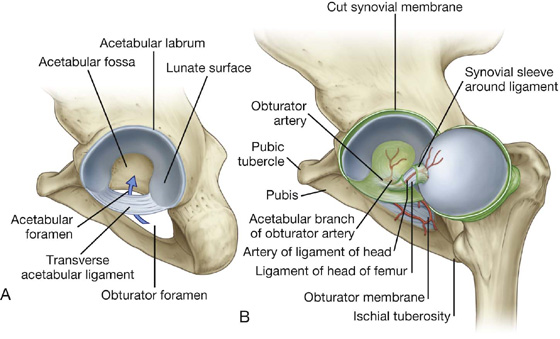
The acetabulum almost entirely encompasses the hemispherical head of the femur and contributes substantially to joint stability. The nonarticular acetabular fossa contains loose connective tissue. The lunate surface is covered by hyaline cartilage and is broadest superiorly (Fig. 6.12).
Except for the fovea, the head of the femur is also covered by hyaline cartilage.
The rim of the acetabulum is raised slightly by a fibrocartilaginous collar (the acetabular labrum). Inferiorly, the labrum bridges across the acetabular notch as the transverse acetabular ligament and converts the notch into a foramen (Fig. 6.12A).
The ligament of head of femur is a flat band of delicate connective tissue that attaches at one end to the fovea on the head of the femur and at the other end to the acetabular fossa, transverse acetabular ligament, and margins of the acetabular notch (Fig. 6.12B). It carries a small branch of the obturator artery, which contributes to the blood supply of the head of the femur.
The synovial membrane attaches to the margins of the articular surfaces of the femur and acetabulum, forms a tubular covering around the ligament of head of femur, and lines the fibrous membrane of the joint (Figs. 6.12B, 6.13). From its attachment to the margin of the head of the femur, the synovial membrane covers the neck of the femur before reflecting onto the fibrous membrane (Fig. 6.13).
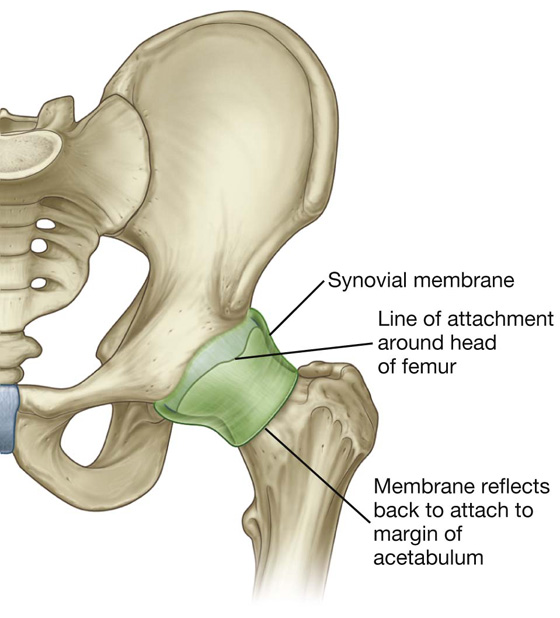
Fig. 6.13 Synovial membrane of the hip joint.
The fibrous membrane that encloses the hip joint is strong and generally thick. Medially, it is attached to the margin of the acetabulum, the transverse acetabular ligament, and the adjacent margin of the obturator foramen (Fig. 6.14A). Laterally, it is attached to the intertrochanteric line on the anterior aspect of the femur and to the neck of the femur just proximal to the intertrochanteric crest on the posterior surface.
Ligaments
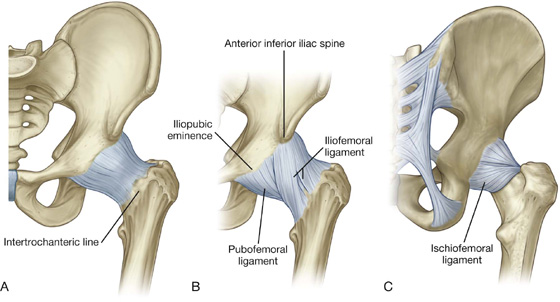
Three ligaments reinforce the external surface of the fibrous membrane and stabilize the joint: the iliofemoral, pubofemoral, and ischiofemoral ligaments.
 The iliofemoral ligament is anterior to the hip joint and is triangular-shaped (Fig. 6.14B). Its apex is attached to the ilium between the anterior inferior iliac spine and the margin of the acetabulum and its base is attached along the intertrochanteric line of the femur. Parts of the ligament attached above and below the intertrochanteric line are thicker than those attached to the central part of the line. This results in the ligament having a Y appearance.
The iliofemoral ligament is anterior to the hip joint and is triangular-shaped (Fig. 6.14B). Its apex is attached to the ilium between the anterior inferior iliac spine and the margin of the acetabulum and its base is attached along the intertrochanteric line of the femur. Parts of the ligament attached above and below the intertrochanteric line are thicker than those attached to the central part of the line. This results in the ligament having a Y appearance.
 The pubofemoral ligament is anteroinferior to the hip joint (Fig. 6.14B). It is also triangular in shape, with its base attached medially to the iliopubic eminence, adjacent bone, and obturator membrane. Laterally, it blends with the fibrous membrane and with the deep surface of the iliofemoral ligament.
The pubofemoral ligament is anteroinferior to the hip joint (Fig. 6.14B). It is also triangular in shape, with its base attached medially to the iliopubic eminence, adjacent bone, and obturator membrane. Laterally, it blends with the fibrous membrane and with the deep surface of the iliofemoral ligament.
 The ischiofemoral ligament reinforces the posterior aspect of the fibrous membrane (Fig. 6.14C). It is attached medially to the ischium, just posteroinferior to the acetabulum, and laterally to the greater trochanter deep to the iliofemoral ligament.
The ischiofemoral ligament reinforces the posterior aspect of the fibrous membrane (Fig. 6.14C). It is attached medially to the ischium, just posteroinferior to the acetabulum, and laterally to the greater trochanter deep to the iliofemoral ligament.
The fibers of all three ligaments are oriented in a spiral fashion around the hip joint so that they become taut when the joint is extended. This stabilizes the joint and reduces the amount of muscle energy required to maintain a standing position.
Blood supply and innervation
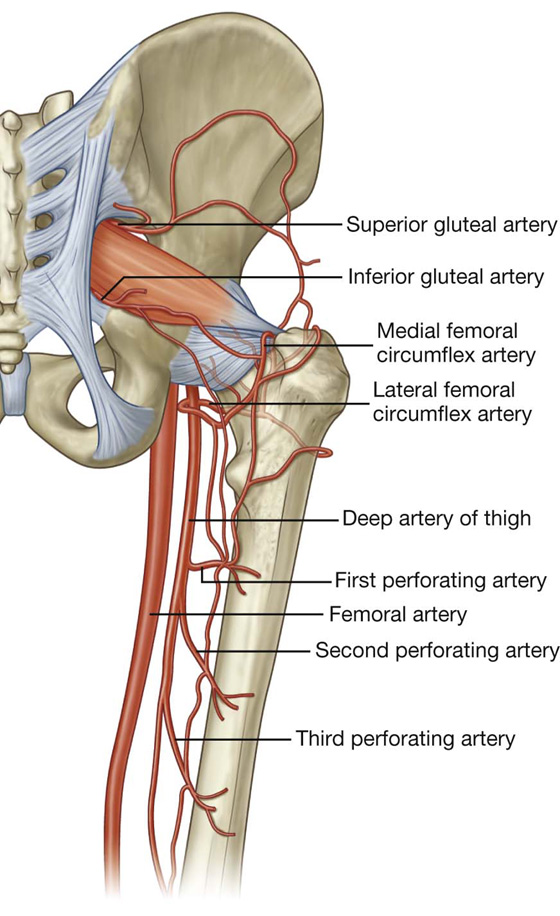
Vascular supply to the hip joint is predominantly through branches of the obturator artery, medial and lateral circumflex femoral arteries, superior and inferior gluteal arteries, and the first perforating branch of the deep artery of the thigh. The articular branches of these vessels form a network around the joint (Fig. 6.15).
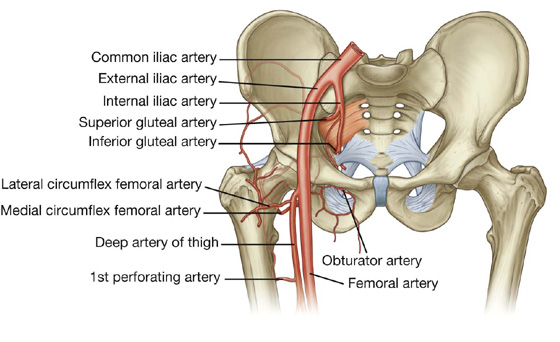
Fig. 6.15 Blood supply of the hip joint.
The hip joint is innervated by articular branches from the femoral, obturator, and superior gluteal nerves, and the nerve to the quadratus femoris.
Imaging app
Visualizing the hip joint
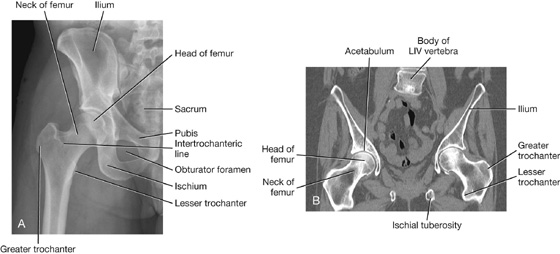
Fig. 6.16 Hip joint. A. Normal hip joint. Radiograph, AP view. B. Hip joints. CT image in coronal plane.
Gateways to the lower limb
There are four major routes by which structures pass from the abdomen and pelvis into and out of the lower limb (Fig. 6.17):
 Obturator canal — an almost vertically oriented passageway at the anterosuperior edge of the obturator foramen. The obturator canal connects the abdominopelvic region with the medial compartment of the thigh.
Obturator canal — an almost vertically oriented passageway at the anterosuperior edge of the obturator foramen. The obturator canal connects the abdominopelvic region with the medial compartment of the thigh. Greater sciatic foramen — formed on the posterolateral pelvic wall and is the major route for structures to pass between the pelvis and the gluteal region of the lower limb (Fig. 6.17). The piriformis muscle passes out of the pelvis into the gluteal region through the greater sciatic foramen and separates the foramen into two parts, a part above the muscle and a part below.
Greater sciatic foramen — formed on the posterolateral pelvic wall and is the major route for structures to pass between the pelvis and the gluteal region of the lower limb (Fig. 6.17). The piriformis muscle passes out of the pelvis into the gluteal region through the greater sciatic foramen and separates the foramen into two parts, a part above the muscle and a part below.
 Lesser sciatic foramen — inferior to the greater sciatic foramen on the posterolateral pelvic wall (Fig. 6.17). It is also inferior to the lateral attachment of the pelvic floor (levator ani and coccygeus muscles) to the pelvic wall and therefore connects the gluteal region with the perineum.
Lesser sciatic foramen — inferior to the greater sciatic foramen on the posterolateral pelvic wall (Fig. 6.17). It is also inferior to the lateral attachment of the pelvic floor (levator ani and coccygeus muscles) to the pelvic wall and therefore connects the gluteal region with the perineum.
 Gap between the inguinal ligament and pelvic bone — a large crescent-shaped gap between the inguinal ligament above and the anterosuperior margin of the pelvic bone below is the major route of communication between the abdomen and the anteromedial aspect of the thigh (Fig. 6.17).
Gap between the inguinal ligament and pelvic bone — a large crescent-shaped gap between the inguinal ligament above and the anterosuperior margin of the pelvic bone below is the major route of communication between the abdomen and the anteromedial aspect of the thigh (Fig. 6.17).
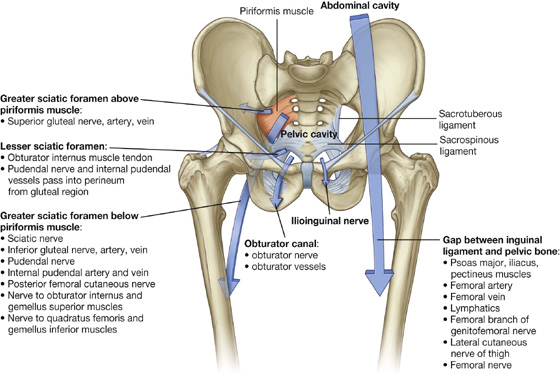
Fig. 6.17 Gateways to the lower limb.
Nerves
Nerves that enter the lower limb from the abdomen and pelvis are terminal branches of the lumbosacral plexus on the posterior wall of the abdomen and the posterolateral walls of the pelvis (Fig. 6.18).
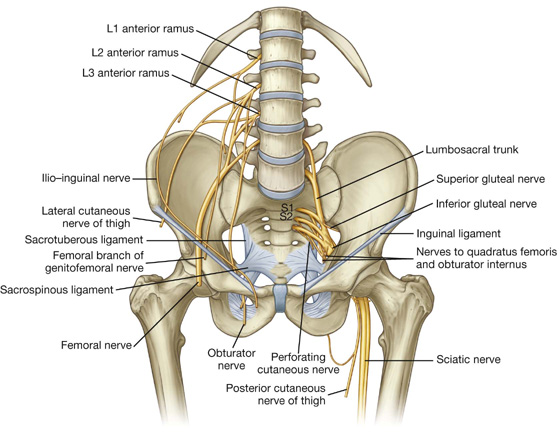
Fig. 6.18 Branches of the lumbosacral plexus.
The lumbar plexus is formed by the anterior rami of spinal nerves L1 to L3 and part of L4. The rest of the anterior ramus of L4 and the anterior ramus of L5 combine to form the lumbosacral trunk, which enters the pelvic cavity and joins with the anterior rami of S1 to S3 and part of S4 to form the sacral plexus.
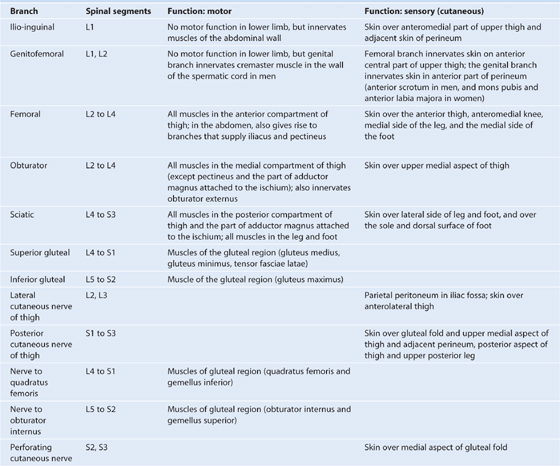
Nerves that originate from the lumbosacral plexus and that leave the abdomen and pelvis to enter the lower limb are indicated in Fig. 6.18 and described in Table 6.1, p. 278.
Table 6.1 Branches of the lumbosacral plexus associated with the lower limb
Arteries
Femoral artery
The major artery supplying the lower limb is the femoral artery (Fig. 6.19), which is the continuation of the external iliac artery in the abdomen. The external iliac artery becomes the femoral artery as the vessel passes under the inguinal ligament to enter the femoral triangle in the anterior aspect of the thigh. Branches supply most of the thigh and all of the leg and foot.
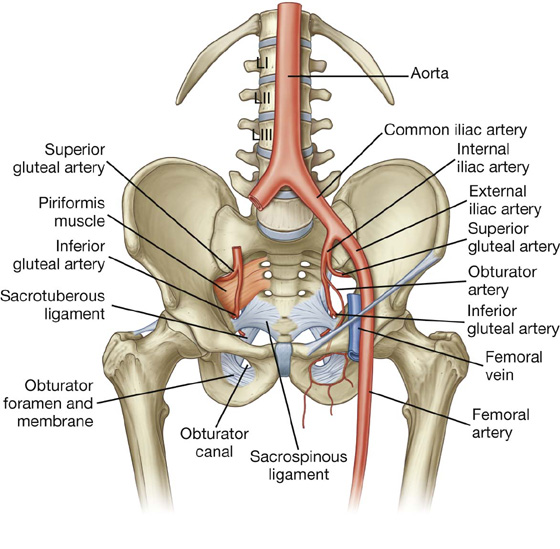
Fig. 6.19 Arteries of the lower limb.
Superior and inferior gluteal arteries and the obturator artery
The superior and inferior gluteal arteries originate in the pelvic cavity as branches of the internal iliac artery (Fig. 6.19, see pp. 240-241) and supply the gluteal region. The superior gluteal artery leaves the pelvis through the greater sciatic foramen above the piriformis muscle and the inferior gluteal artery leaves through the same foramen, but below the piriformis muscle.
The obturator artery is also a branch of the internal iliac artery in the pelvic cavity (p. 241) and passes through the obturator canal to enter and supply the medial compartment of the thigh (Fig. 6.19).
Branches of the femoral, inferior gluteal, superior gluteal, and obturator arteries, together with branches from the internal pudendal artery of the perineum, interconnect to form an anastomotic network in the upper thigh and gluteal region. The presence of these anastomotic channels may provide collateral circulation when one of the vessels is interrupted.
Veins
Veins draining the lower limb form superficial and deep groups (Fig. 6.20).
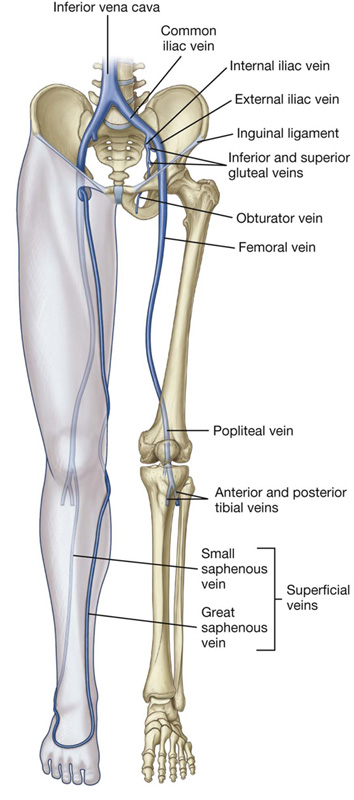
Fig. 6.20 Veins of the lower limb.
The deep veins generally follow the arteries (femoral, superior gluteal, inferior gluteal, and obturator). The major deep vein draining the limb is the femoral vein (Fig. 6.20). It becomes the external iliac vein when it passes under the inguinal ligament to enter the abdomen.
The superficial veins are in the subcutaneous connective tissue and are interconnected with and ultimately drain into the deep veins. The superficial veins form two major channels—the great saphenous vein and the small saphenous vein. Both veins originate from a dorsal venous arch in the foot (Fig. 6.20):
 The great saphenous vein originates from the medial side of the dorsal venous arch, and then ascends up the medial side of the leg, knee, and thigh to connect with the femoral vein just inferior to the inguinal ligament.
The great saphenous vein originates from the medial side of the dorsal venous arch, and then ascends up the medial side of the leg, knee, and thigh to connect with the femoral vein just inferior to the inguinal ligament.
 The small saphenous vein originates from the lateral side of the dorsal venous arch, ascends up the posterior surface of the leg, and then penetrates deep fascia to join the popliteal vein posterior to the knee; proximal to the knee, the popliteal vein becomes the femoral vein.
The small saphenous vein originates from the lateral side of the dorsal venous arch, ascends up the posterior surface of the leg, and then penetrates deep fascia to join the popliteal vein posterior to the knee; proximal to the knee, the popliteal vein becomes the femoral vein.Clinical app
Varicose veins
The normal flow of blood in the venous system depends on the presence of competent valves, which prevent reflux. Venous return is supplemented with contraction of the muscles in the lower limb, which pump the blood toward the heart. When venous valves become incompetent they tend to place extra pressure on more distal valves, which may also become incompetent. This condition produces dilated tortuous superficial veins (varicose veins) in the distribution of the great (long) and small (short) saphenous venous systems.
Clinical app
Deep vein thrombosis
Thrombosis resulting from venous stasis, injury to the vessel wall, or hypercoagulable states may occur in the deep veins of the lower limb and within the pelvic veins.
In some patients a deep vein thrombosis (DVT) in the veins of the leg may propagate into the femoral veins. This clot may break off and pass through the heart to enter the pulmonary circulation, resulting in occlusion of the pulmonary artery (pulmonary embolism), cardiopulmonary arrest, and death.
Clinical app
Harvesting veins for grafts
Vein grafts have long been used for vascular conduits. Superficial veins of the arms and legs are harvested and used to bypass areas of arterial occlusion and stenoses. Typically vein bypass grafts are used for coronary artery bypass surgery and to bypass areas of vascular occlusion in the lower limb.
The commonest vein used for bypass grafting is the great saphenous vein. A long incision is required to obtain access to the vein and after tributaries of the vein are ligated, the vein is removed.
It is important to remember that veins contain valves and in order to use the vein as an appropriate conduit, it must either be reversed or, using special surgical techniques, the valves can be obliterated.
In coronary artery bypass grafting the vein is anastomosed to the ascending arch of the aorta and then anastomosed distal to the regions of occlusion on the coronary vessels. Similarly, in lower limb ischemic disease the vein can be used to bypass the regions of stenosis and occlusion within the femoral artery and the distal branches.
Lymphatics
Most lymphatic vessels in the lower limb drain into superficial and deep inguinal nodes located in the fascia just inferior to the inguinal ligament (Fig. 6.21).
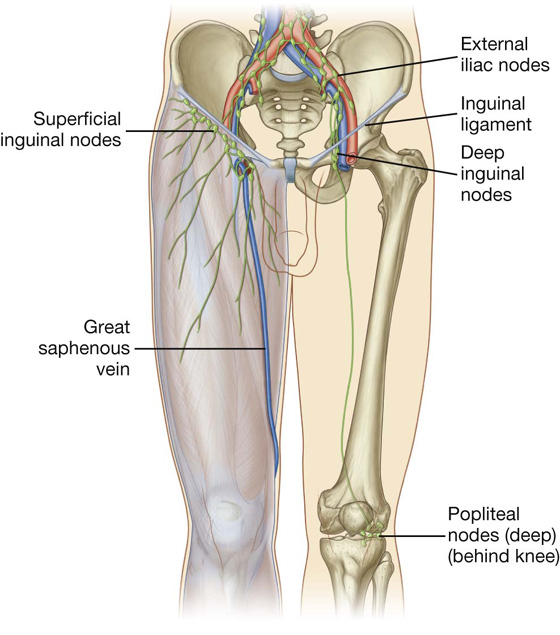
Fig. 6.21 Lymphatic drainage of the lower limb.
Superficial inguinal nodes
The superficial inguinal nodes, approximately 10 in number, are in the superficial fascia and parallel the course of the inguinal ligament in the upper thigh (Fig. 6.21). Medially, they extend inferiorly along the terminal part of the great saphenous vein.
Superficial inguinal nodes receive lymph from the gluteal region, lower abdominal wall, perineum, and superficial regions of the lower limb. They drain, via vessels that accompany the femoral vessels, into external iliac nodes associated with the external iliac artery in the abdomen.
Deep inguinal nodes
The deep inguinal nodes, up to three in number, are medial to the femoral vein (Fig. 6.21).
Popliteal nodes
In addition to the inguinal nodes, there is a small collection of deep nodes posterior to the knee close to the popliteal vessels (Fig. 6.21). These popliteal nodes receive lymph from superficial vessels, which accompany the small saphenous vein, and from deep areas of the leg and foot. They ultimately drain into the deep and superficial inguinal nodes.
Deep fascia and the saphenous opening
Fascia lata
The outer layer of deep fascia in the lower limb forms a thick “stocking-like” membrane, which covers the limb and lies beneath the superficial fascia (Fig. 6.22A). This deep fascia is particularly thick in the thigh and gluteal region and is termed the fascia lata.
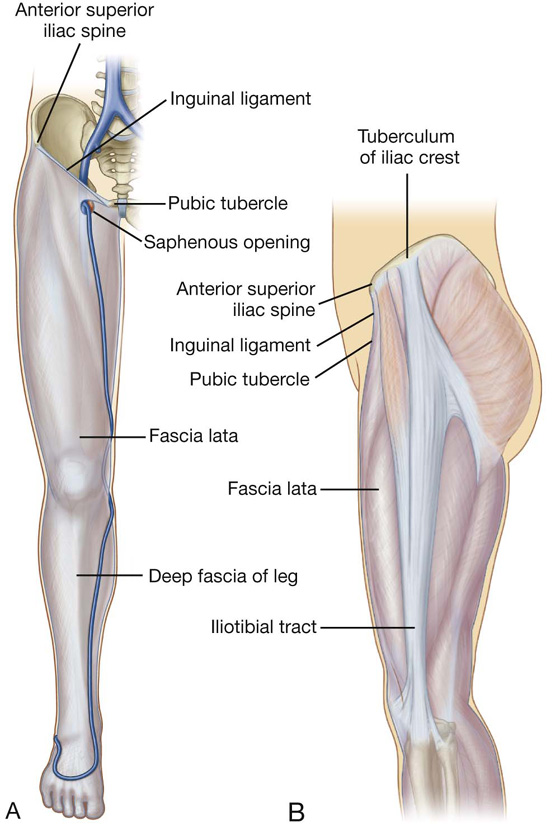
Fig. 6.22 Fascia lata. A. Right limb. Anterior view. B. Left limb. Lateral view.
The fascia lata is anchored superiorly to bone and soft tissues along a line of attachment that defines the upper margin of the lower limb.
Inferiorly, the fascia lata is continuous with the deep fascia of the leg.
Iliotibial tract
The fascia lata is thickened laterally into a longitudinal band (the iliotibial tract), which descends along the lateral margin of the limb from the tuberculum of iliac crest to a bony attachment just below the knee (Fig. 6.22B).
The superior aspect of the fascia lata in the gluteal region splits anteriorly to enclose the tensor fasciae latae muscle and posteriorly to enclose the gluteus maximus muscle:
 The tensor fasciae latae muscle is partially enclosed by and inserts into the superior and anterior aspects of the iliotibial tract.
The tensor fasciae latae muscle is partially enclosed by and inserts into the superior and anterior aspects of the iliotibial tract. Most of the gluteus maximus muscle inserts into the posterior aspect of the iliotibial tract.
Most of the gluteus maximus muscle inserts into the posterior aspect of the iliotibial tract.
The tensor fasciae latae and gluteus maximus muscles, working through their attachments to the iliotibial tract, hold the leg in extension once other muscles have extended the leg at the knee joint. The iliotibial tract and its two associated muscles also stabilize the hip joint by preventing lateral displacement of the proximal end of the femur away from the acetabulum.
Saphenous opening
The fascia lata has one prominent aperture on the anterior aspect of the thigh just inferior to the medial end of the inguinal ligament (the saphenous opening), which allows the great saphenous vein to pass from superficial fascia through the deep fascia to connect with the femoral vein (Fig. 6.23).
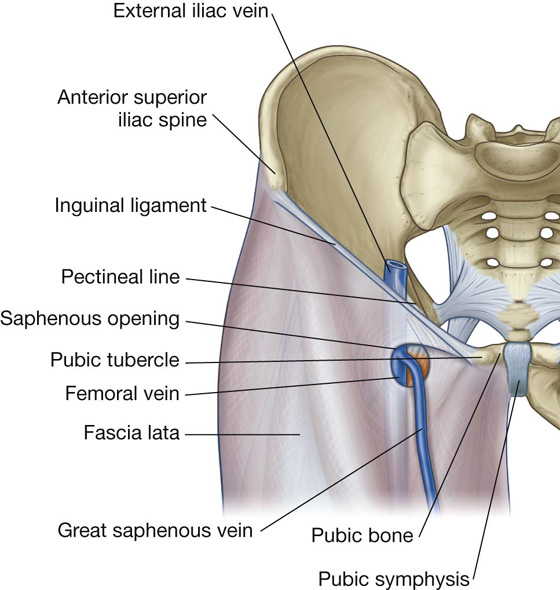
Fig. 6.23 Saphenous opening. Anterior view.
Femoral triangle
The femoral triangle is a wedge-shaped depression formed by muscles in the upper thigh at the junction between the anterior abdominal wall and the lower limb (Fig. 6.24):
 The base of the triangle is the inguinal ligament.
The base of the triangle is the inguinal ligament.
 The medial border is the medial margin of the adductor longus muscle in the medial compartment of the thigh.
The medial border is the medial margin of the adductor longus muscle in the medial compartment of the thigh. The lateral margin is the medial margin of the sartorius muscle in the anterior compartment of the thigh.
The lateral margin is the medial margin of the sartorius muscle in the anterior compartment of the thigh. The floor of the triangle is formed medially by the pectineus and adductor longus muscles in the medial compartment of the thigh and laterally by the iliopsoas muscle descending from the abdomen.
The floor of the triangle is formed medially by the pectineus and adductor longus muscles in the medial compartment of the thigh and laterally by the iliopsoas muscle descending from the abdomen. The apex of the femoral triangle points inferiorly and is continuous with a fascial canal (adductor canal), which descends medially down the thigh and posteriorly through an aperture in the lower end of one of the largest of the adductor muscles in the thigh (the adductor magnus muscle) to open into the popliteal fossa behind the knee.
The apex of the femoral triangle points inferiorly and is continuous with a fascial canal (adductor canal), which descends medially down the thigh and posteriorly through an aperture in the lower end of one of the largest of the adductor muscles in the thigh (the adductor magnus muscle) to open into the popliteal fossa behind the knee.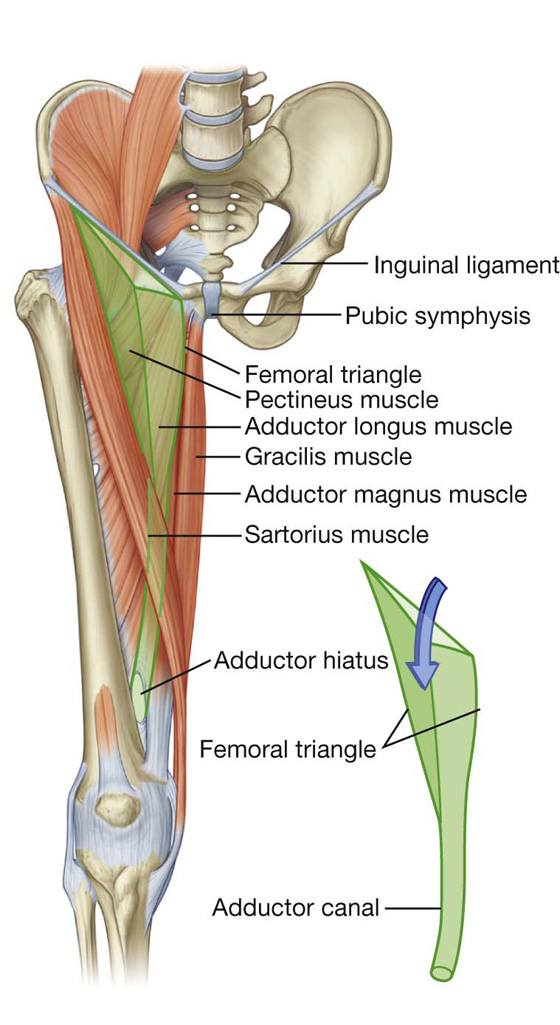
Fig. 6.24 Boundaries of the femoral triangle.
The femoral nerve, artery, and vein, and lymphatics pass between the abdomen and lower limb under the inguinal ligament and in the femoral triangle (Fig. 6.25). The femoral artery and vein pass inferiorly through the adductor canal and become the popliteal vessels behind the knee where they meet and are distributed with branches of the sciatic nerve, which descends through the posterior thigh from the gluteal region.
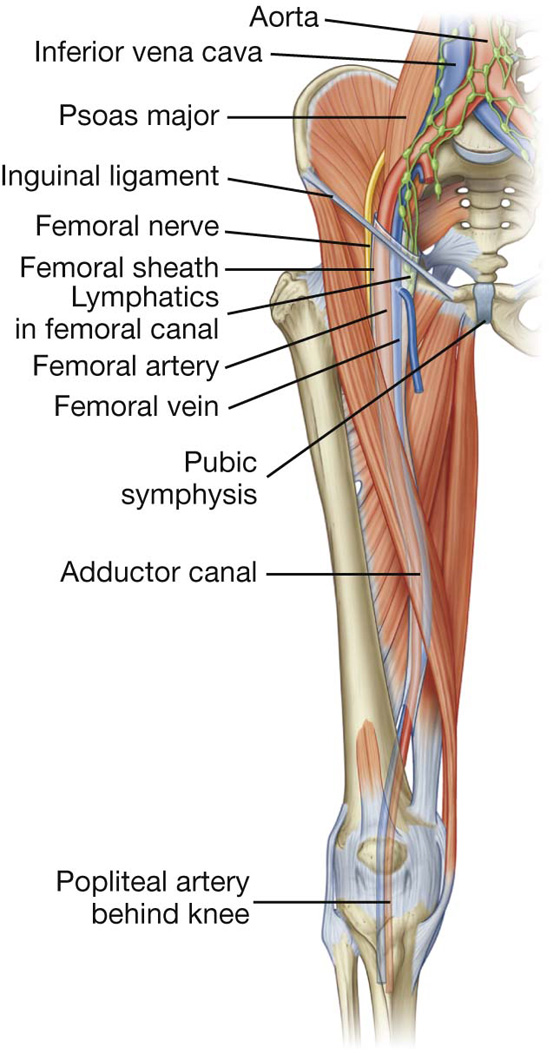
Fig. 6.25 Contents of the femoral triangle.
From lateral to medial, major structures in the femoral triangle are the femoral nerve, the femoral artery, the femoral vein, and lymphatic vessels (Fig. 6.25).
Femoral sheath
In the femoral triangle, the femoral artery and vein and the associated lymphatic vessels are surrounded by a funnel-shaped sleeve of fascia (the femoral sheath) (Fig. 6.25). The sheath is continuous superiorly with the transversalis fascia and iliacus fascia of the abdomen and merges inferiorly with connective tissue associated with the vessels. Each of the three structures surrounded by the sheath is contained within a separate fascial compartment within the sheath. The most medial compartment (the femoral canal) contains the lymphatic vessels and is conical in shape. The opening of this canal superiorly is potentially a weak point in the lower abdomen and is the site for femoral hernias. The femoral nerve is lateral to and not contained within the femoral sheath.
Surface anatomy
Finding the femoral artery in the femoral triangle
The femoral artery descends into the thigh from the abdomen by passing under the inguinal ligament and into the femoral triangle (Fig. 6.26). In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the pubic symphysis and the anterior superior iliac spine. Medial to the artery is the femoral vein and medial to the vein is the femoral canal, which contains lymphatics and lies immediately lateral to the pubic tubercle. The femoral nerve lies lateral to the femoral artery.

Fig. 6.26 Position of the femoral artery in the femoral triangle.
Clinical app
Vascular access in the lower limb
The femoral artery and vein are easily accessible in the femoral triangle.
Many radiological procedures involve catheterization of the femoral artery or the femoral vein to obtain access to the contralateral lower limb, the ipsilateral lower limb, the vessels of the thorax and abdomen, and even the cerebral vessels.
Cardiologists also can use the femoral artery to place catheters in vessels around the arch of the aorta and into the coronary arteries to perform coronary angiography and angioplasty.
GLUTEAL REGION
The gluteal region lies posterolateral to the bony pelvis and the proximal end of the femur (Fig. 6.27). Muscles in the region mainly abduct, extend, and laterally rotate the femur relative to the pelvic bone.
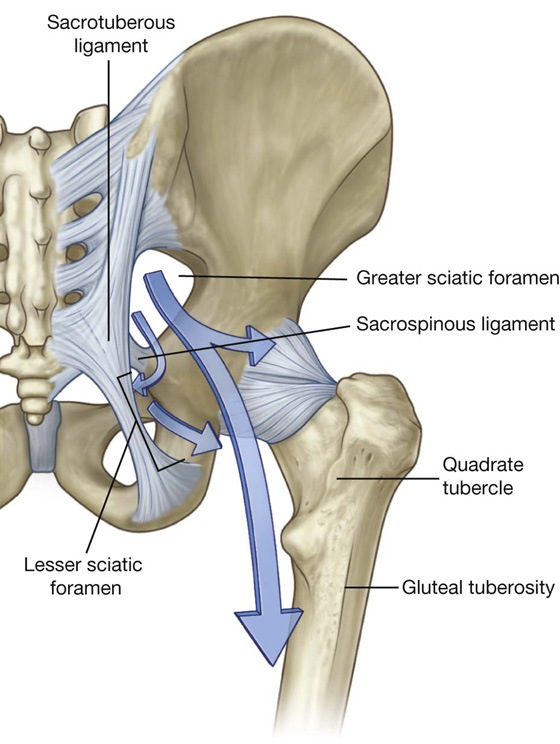
Fig. 6.27 Gluteal region. Posterior view.
The gluteal region communicates anteromedially with the pelvic cavity and perineum through the greater and lesser sciatic foramina, respectively (Fig. 6.27). Inferiorly, it is continuous with the posterior thigh.
Muscles
Muscles of the gluteal region (Table 6.2, Fig. 6.28) compose mainly two groups:
 a deep group of small muscles, which are mainly lateral rotators of the femur at the hip joint and include the piriformis, obturator internus, gemellus superior, gemellus inferior, and quadratus femoris;
a deep group of small muscles, which are mainly lateral rotators of the femur at the hip joint and include the piriformis, obturator internus, gemellus superior, gemellus inferior, and quadratus femoris; a more superficial group of larger muscles, which mainly abduct and extend the hip and include the gluteus minimus, gluteus medius, and gluteus maximus. An additional muscle in this group, the tensor fasciae latae, stabilizes the knee in extension by acting on a specialized longitudinal band of deep fascia (the iliotibial tract) that passes down the lateral side of the thigh to attach to the proximal end of the tibia in the leg.
a more superficial group of larger muscles, which mainly abduct and extend the hip and include the gluteus minimus, gluteus medius, and gluteus maximus. An additional muscle in this group, the tensor fasciae latae, stabilizes the knee in extension by acting on a specialized longitudinal band of deep fascia (the iliotibial tract) that passes down the lateral side of the thigh to attach to the proximal end of the tibia in the leg.Table 6.2 Muscles of the gluteal region (spinal segments in bold are the major segments innervating the muscle)
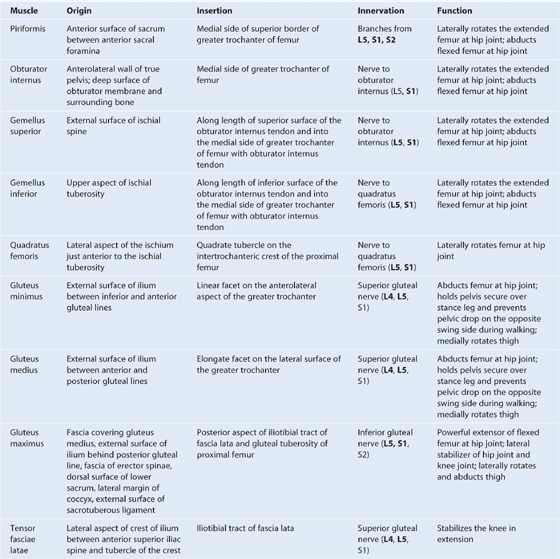
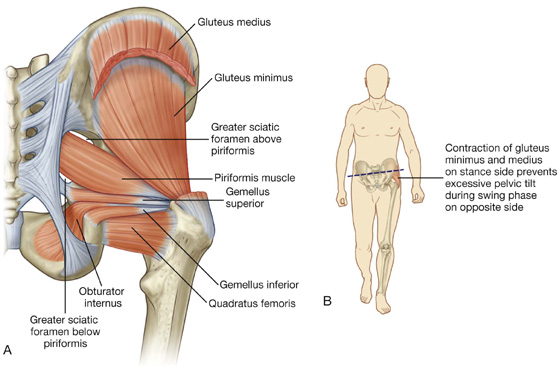
Fig. 6.28 Deep muscles in the gluteal region. A. Posterior view. B. Function.
The piriformis muscle is the most superior of the deep group of muscles (Fig. 6.28A) and is a muscle of the pelvic wall and of the gluteal region. It originates from between the anterior sacral foramina on the anterolateral surface of the sacrum and passes laterally and inferiorly through the greater sciatic foramen. Piriformis is an important landmark because it divides the greater sciatic foramen into two regions, one above and one below the piriformis.
The obturator internus muscle, like the piriformis muscle, is a muscle of the pelvic wall and of the gluteal region (Fig. 6.28A). The muscle fibers of the obturator internus converge to form a tendon, which bends 90° around the ischium between the ischial spine and ischial tuberosity, and passes through the lesser sciatic foramen to enter the gluteal region. Gemellus superior and inferior (gemelli is Latin for “twins”) are a pair of triangular muscles associated with the upper and lower margins of the obturator internus tendon (Fig. 6.28A).
The gluteus medius and minimus muscles abduct the pelvis over the stance limb at the hip joint and reduce pelvic drop over the opposite swing limb during walking (Fig. 6.28B).
Clinical app
Trendelenburg’s sign
Trendelenburg’s sign occurs in people with weak or paralyzed abductor muscles (gluteus medius and gluteus minimus) of the hip. The sign is demonstrated by asking the patient to stand on one limb. When standing on the affected limb, the pelvis severely drops over the swing limb.
Positive findings are typically found in patients with damage to the superior gluteal nerve. Damage to this nerve may occur with associated pelvic fractures, space occupying lesions within the pelvis extending into the greater sciatic foramen and in some cases relating to hip surgery where there has been atrophy and disruption of the insertion of the gluteus medius and gluteus minimus tendons on the greater trochanter.
In patients with a positive Trendelenburg’s sign, gait also is abnormal. Typically during the stance phase of the affected limb, the weakened abductor muscles allow the pelvis to tilt inferiorly over the swing limb. The patient compensates for the pelvic drop by lurching the trunk to the affected side in order to maintain the level of the pelvis throughout the gait cycle.
Gluteus maximus is the largest muscle in the gluteal region and overlies most of the other gluteal muscles (Fig. 6.29). It is quadrangular in shape and has a broad origin from the bony pelvis and associated ligaments and fascia. It is often described as being enclosed within two layers of the fascia lata, which covers the thigh and gluteal region. Laterally, the upper and superficial lower parts of the gluteus maximus insert into the iliotibial tract, which passes over the lateral surface of the greater trochanter and descends down the thigh and into the upper leg. Deep distal parts of the muscle attach to the elongate gluteal tuberosity of the proximal femur.
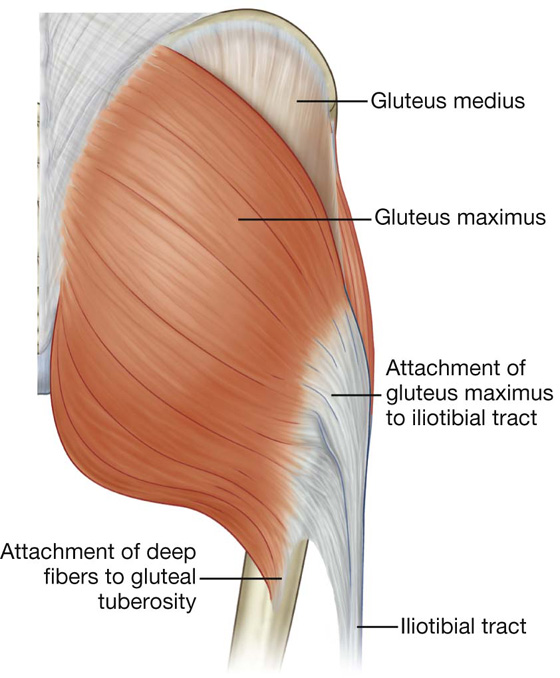
Fig. 6.29 Gluteus maximus muscle. Posterior view.
Nerves
Superior gluteal nerve
Of all the nerves that pass through the greater sciatic foramen, the superior gluteal nerve is the only one that passes above the piriformis muscle (Fig. 6.30A). After entering the gluteal region, the nerve loops up over the inferior margin of gluteus minimus and travels anteriorly and laterally in the plane between the gluteus minimus and medius muscles.
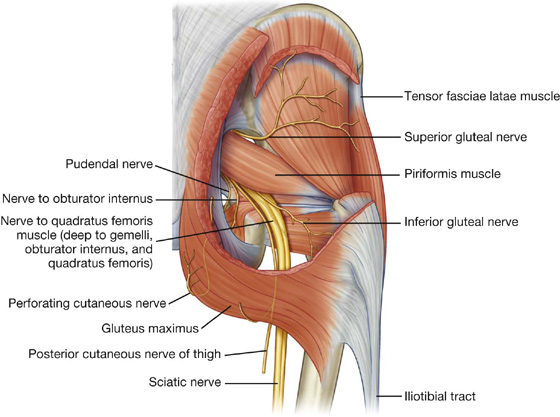
Fig. 6.30 Nerves of the gluteal region.
The superior gluteal nerve supplies branches to the gluteus minimus and medius muscles and terminates by innervating the tensor fasciae latae muscle.
Sciatic nerve
The sciatic nerve enters the gluteal region through the greater sciatic foramen inferior to the piriformis muscle (Fig. 6.30A). It descends in the plane between the superficial and deep group of gluteal region muscles, crossing the posterior surfaces of first the obturator internus and associated gemellus muscles and then the quadratus femoris muscle. It lies just deep to the gluteus maximus at the midpoint between the ischial tuberosity and the greater trochanter. At the lower margin of the quadratus femoris muscle, the sciatic nerve enters the posterior thigh.
The sciatic nerve is the largest nerve in the body and innervates all muscles in the posterior compartment of the thigh that flex the knee and all muscles that work the ankle and foot. It also innervates a large area of skin in the lower limb.
Nerve to quadratus femoris
The nerve to the quadratus femoris enters the gluteal region through the greater sciatic foramen inferior to the piriformis muscle and deep to the sciatic nerve (Fig. 6.30). Unlike other nerves in the gluteal region, the nerve to the quadratus femoris lies anterior to the plane of the deep muscles.
The nerve to the quadratus femoris descends along the ischium deep to the tendon of the obturator internus muscle and associated gemellus muscles to penetrate and innervate the quadratus femoris. It supplies a small branch to the gemellus inferior.
Nerve to obturator internus
The nerve to the obturator internus enters the gluteal region through the greater sciatic foramen inferior to the piriformis muscle and between the posterior cutaneous nerve of the thigh and the pudendal nerve (Fig. 6.30). It supplies a small branch to the gemellus superior and then passes over the ischial spine and through the lesser sciatic foramen to innervate the obturator internus muscle from the medial surface of the muscle in the perineum.
Posterior cutaneous nerve of the thigh
The posterior cutaneous nerve of the thigh enters the gluteal region through the greater sciatic foramen inferior to the piriformis muscle and immediately medial to the sciatic nerve (Fig. 6.30). It descends through the gluteal region just deep to the gluteus maximus and enters the posterior thigh.
The posterior cutaneous nerve of the thigh has a number of gluteal branches, which loop around the lower margin of the gluteus maximus muscle to innervate skin over the gluteal fold. A small perineal branch passes medially to contribute to the innervation of skin of the scrotum or labia majora in the perineum. The main trunk of the posterior cutaneous nerve of the thigh passes inferiorly, giving rise to branches that innervate skin on the posterior thigh and leg.
Pudendal nerve
The pudendal nerve enters the gluteal region through the greater sciatic foramen inferior to the piriformis muscle and medial to the sciatic nerve (Fig. 6.30). It passes over the sacrospinous ligament and immediately passes through the lesser sciatic foramen to enter the perineum. The course of the pudendal nerve in the gluteal region is short and the nerve is often hidden by the overlying upper margin of the sacrotuberous ligament.
The pudendal nerve is the major somatic nerve of the perineum and has no branches in the gluteal region.
Inferior gluteal nerve
The inferior gluteal nerve enters the gluteal region through the greater sciatic foramen inferior to the piriformis muscle and along the posterior surface of the sciatic nerve (Fig. 6.30). It penetrates and supplies the gluteus maximus muscle.
Perforating cutaneous nerve
The perforating cutaneous nerve is the only nerve in the gluteal region that does not enter the area through the greater sciatic foramen. It is a small nerve that leaves the sacral plexus in the pelvic cavity by piercing the sacrotuberous ligament. It then loops around the lower border of the gluteus maximus to supply skin over the medial aspect of the gluteus maximus (Fig. 6.30).
Clinical app
Intramuscular injection in the gluteal region: avoiding the sciatic nerve
From time to time it is necessary to administer drugs intramuscularly; that is, by direct injection into muscles. This procedure must be carried out without injuring neurovascular structures. A typical site for an intramuscular injection is the gluteal region. The sciatic nerve passes through this region and needs to be avoided. The safest place to inject is the upper outer quadrant of either gluteal region.
The gluteal region can be divided into quadrants by two imaginary lines positioned using palpable bony landmarks (Fig. 6.31).
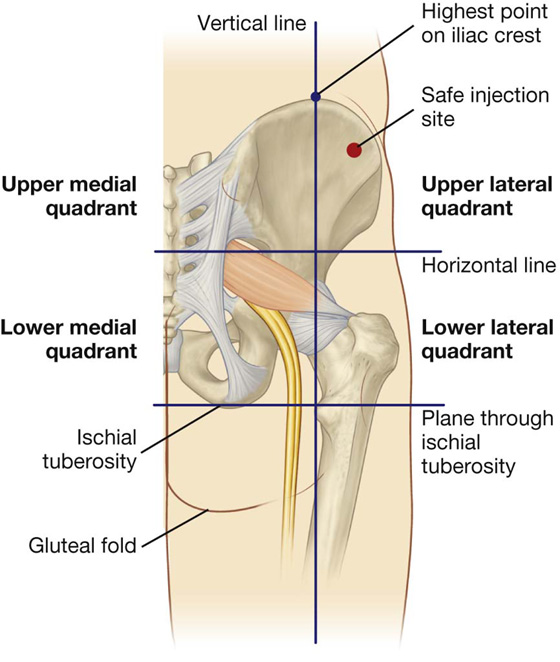
Fig. 6.31 Site for intramuscular injections.
One line descends vertically from the highest point of the iliac crest.
The other line passes horizontally through the first line midway between the highest point of the iliac crest and the horizontal plane through the ischial tuberosity.
It is important to remember that the gluteal region extends as far forward as the anterior superior iliac spine. The sciatic nerve curves through the upper lateral corner of the lower medial quadrant and descends along the medial margin of the lower lateral quadrant.
Occasionally, the sciatic nerve bifurcates into its tibial and common fibular branches in the pelvis, in which case the common fibular nerve passes into the gluteal region through, or even above, the piriformis muscle.
The anterior corner of the upper lateral quadrant is normally used for injections to avoid injuring any part of the sciatic nerve or other nerves and vessels in the gluteal region. A needle placed in this region enters the gluteus medius anterosuperior to the margin of the gluteus maximus.
Arteries
Inferior gluteal artery
The inferior gluteal artery originates from the anterior trunk of the internal iliac artery in the pelvic cavity. It leaves the pelvic cavity through the greater sciatic foramen inferior to the piriformis muscle (Fig. 6.32).
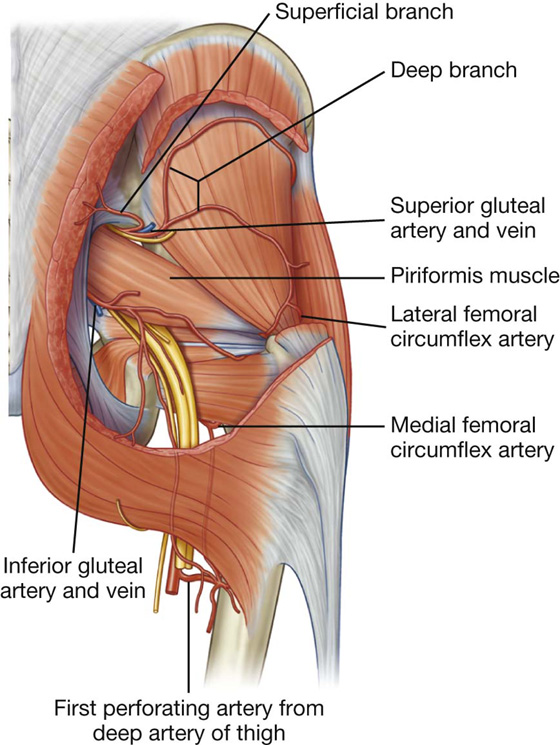
Fig. 6.32 Arteries of the gluteal region.
The inferior gluteal artery supplies adjacent muscles and descends through the gluteal region and into the posterior thigh where it supplies adjacent structures and anastomoses with perforating branches of the femoral artery. It also supplies a branch to the sciatic nerve.
Superior gluteal artery
The superior gluteal artery originates from the posterior trunk of the internal iliac artery in the pelvic cavity. It leaves the pelvic cavity through the greater sciatic foramen above the piriformis muscle (Fig. 6.32). In the gluteal region, it divides into a superficial branch and a deep branch:
 The superficial branch passes onto the deep surface of the gluteus maximus muscle.
The superficial branch passes onto the deep surface of the gluteus maximus muscle.
 The deep branch passes between the gluteus medius and minimus muscles.
The deep branch passes between the gluteus medius and minimus muscles.
In addition to adjacent muscles, the superior gluteal artery contributes to the supply of the hip joint. Branches of the artery also anastomose with the lateral and medial femoral circumflex arteries from the deep femoral artery in the thigh, and with the inferior gluteal artery (Fig. 6.33).
Veins
Inferior and superior gluteal veins follow the inferior and superior gluteal arteries into the pelvis where they join the pelvic plexus of veins. Peripherally, the veins anastomose with superficial gluteal veins, which ultimately drain anteriorly into the femoral vein.
Lymphatics
Deep lymphatic vessels of the gluteal region accompany the blood vessels into the pelvic cavity and connect with internal iliac nodes.
Superficial lymphatics drain into the superficial inguinal nodes on the anterior aspect of the thigh.
THIGH
The thigh is the region of the lower limb that is approximately between the hip and knee joints (Fig. 6.34):
 Anteriorly, it is separated from the abdominal wall by the inguinal ligament.
Anteriorly, it is separated from the abdominal wall by the inguinal ligament.
 Posteriorly, it is separated from the gluteal region by the gluteal fold superficially, and by the inferior margins of the gluteus maximus and quadratus femoris on deeper planes.
Posteriorly, it is separated from the gluteal region by the gluteal fold superficially, and by the inferior margins of the gluteus maximus and quadratus femoris on deeper planes.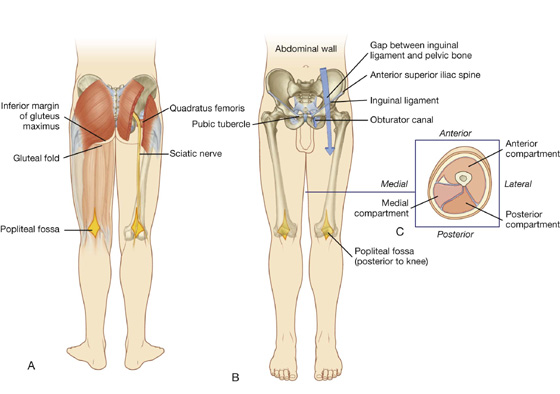
Fig. 6.34 Thigh. A. Posterior view. B. Anterior view. C. Cross-section through the midthigh.
Structures enter and leave the top of the thigh by three routes:
 Posteriorly, the thigh is continuous with the gluteal region and the major structure passing between the two regions is the sciatic nerve (Fig. 6.34A).
Posteriorly, the thigh is continuous with the gluteal region and the major structure passing between the two regions is the sciatic nerve (Fig. 6.34A).
 Anteriorly, the thigh communicates with the abdominal cavity through the aperture between the inguinal ligament and pelvic bone (Fig. 6.34B), and major structures passing through this aperture are the iliopsoas and pectineus muscles, the femoral nerve, artery and vein, and lymphatic vessels.
Anteriorly, the thigh communicates with the abdominal cavity through the aperture between the inguinal ligament and pelvic bone (Fig. 6.34B), and major structures passing through this aperture are the iliopsoas and pectineus muscles, the femoral nerve, artery and vein, and lymphatic vessels.
 Medially, structures (including the obturator nerve and associated vessels) pass between the thigh and pelvic cavity through the obturator canal (Fig. 6.34B).
Medially, structures (including the obturator nerve and associated vessels) pass between the thigh and pelvic cavity through the obturator canal (Fig. 6.34B).
The thigh is divided into three compartments (anterior, medial, and posterior) by intermuscular septa between the posterior aspect of the femur and the fascia lata (the thick layer of deep fascia that completely surrounds or invests the thigh; Fig. 6.34C).
Bones
The skeletal support for the thigh is the femur (Fig. 6.35). Most of the large muscles in the thigh insert into the proximal ends of the two bones of the leg (tibia and fibula), and flex and extend the leg at the knee joint. The distal end of the femur provides origin for the gastrocnemius muscles, which are predominantly in the posterior compartment of the leg and plantarflex the foot.
Shaft and distal end of femur
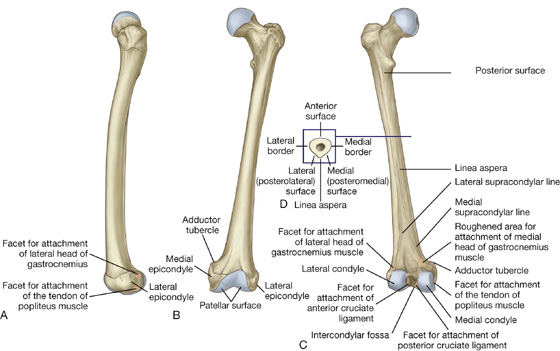
The shaft of femur is bowed forward and has an oblique course from the neck of the femur to the distal end (Fig. 6.35A, B). As a consequence of this oblique orientation, the knee is close to the midline under the body’s center of gravity.
The middle part of the shaft of femur is triangular in cross-section (Fig. 6.35D). In the middle part of the shaft, the femur has smooth medial (posteromedial), lateral (posterolateral), and anterior surfaces and medial, lateral, and posterior borders. The medial and lateral borders are rounded, whereas the posterior border forms a broad roughened crest—the linea aspera (Fig. 6.35C).
In proximal and distal regions of the femur, the linea aspera widens to form an additional posterior surface. At the distal end of the femur, this posterior surface forms the floor of the popliteal fossa and its margins, which are continuous with the linea aspera above, form the medial and lateral supracondylar lines. The medial supracondylar line terminates at a prominent tubercle (the adductor tubercle) on the superior aspect of the medial condyle of the distal end. Just lateral to the lower end of the medial supracondylar line is an elongate roughened area of bone for the proximal attachment of the medial head of the gastrocnemius muscle (Fig. 6.35).
The distal end of femur is characterized by two large condyles, which articulate with the proximal head of the tibia (Fig. 6.35). The condyles are separated posteriorly by an intercondylar fossa and are joined anteriorly where they articulate with the patella.
The surfaces of the condyles that articulate with the tibia are rounded posteriorly and become flatter inferiorly. On each condyle, a shallow oblique groove separates the surface that articulates with the tibia from the more anterior surface that articulates with the patella. The surfaces of the medial and lateral condyles that articulate with the patella form a V-shaped trench, which faces anteriorly. The lateral surface of the trench is larger and steeper than the medial surface.
The walls of the intercondylar fossa bear two facets for the superior attachment of the cruciate ligaments, which stabilize the knee joint (Fig. 6.35C).
Epicondyles, for the attachment of collateral ligaments of the knee joint, are bony elevations on the nonarticular outer surfaces of the condyles (Fig. 6.35).
Additionally, just posterosuperior to the medial epicondyle is the adductor tubercle and just posterior to the lateral epicondyle are facets for the attachment of the lateral head of the gastrocnemius and the popliteus muscles (Fig. 6.35C).
Patella
The patella (knee cap) is the largest sesamoid bone (a bone formed within the tendon of a muscle) in the body and is formed within the tendon of the quadriceps femoris muscle as it crosses anterior to the knee joint to insert on the tibia.
The patella is triangular (Fig. 6.36):
 Its apex is pointed inferiorly for attachment to the patellar ligament, which connects the patella to the tibia.
Its apex is pointed inferiorly for attachment to the patellar ligament, which connects the patella to the tibia. Its base is broad and thick for the attachment of the quadriceps femoris muscle from above.
Its base is broad and thick for the attachment of the quadriceps femoris muscle from above.
 Its posterior surface articulates with the femur and has medial and lateral facets (Fig. 6.36B), which slope away from a raised smooth ridge—the lateral facet is larger than the medial facet for articulation with the larger corresponding surface on the lateral condyle of the femur.
Its posterior surface articulates with the femur and has medial and lateral facets (Fig. 6.36B), which slope away from a raised smooth ridge—the lateral facet is larger than the medial facet for articulation with the larger corresponding surface on the lateral condyle of the femur.
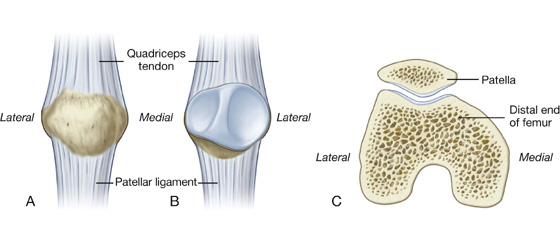
Fig. 6.36 Patella. A. Anterior view. B. Posterior view. C. Superior view.
Proximal end of tibia
The tibia is the medial and larger of the two bones in the leg, and is the only one that articulates with the femur at the knee joint.
The proximal end of the tibia is expanded in the transverse plane for weight bearing and consists of a medial condyle and a lateral condyle, which are both flattened in the horizontal plane and overhang the shaft (Fig. 6.37).
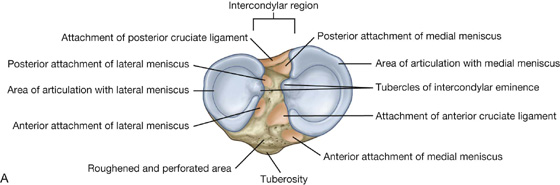
The superior surfaces of the medial and lateral condyles are articular and separated by an intercondylar region, which contains sites of attachment for the cruciate ligaments and interarticular cartilages (menisci) of the knee joint (Fig. 6.37A).
The articular surfaces of the medial and lateral condyles and the intercondylar region together form a “tibial plateau,” which articulates with and is anchored to the distal end of the femur. Inferior to the condyles on the proximal part of the shaft is a large tibial tuberosity and the roughening for muscle and ligament attachments.
Tibial condyles and intercondylar areas
The tibial condyles are thick horizontal discs of bone attached to the top of the tibial shaft (Fig. 6.37).
The medial condyle is larger than the lateral condyle and is better supported over the shaft of the tibia. Its superior surface is oval for articulation with the medial condyle of the femur (Fig. 6.37A). The articular surface extends laterally onto the side of the raised medial intercondylar tubercle.
The superior surface of the lateral condyle is circular and articulates above with the lateral condyle of the femur (Fig. 6.37A). The medial edge of this surface extends onto the side of the lateral intercondylar tubercle.
The superior articular surfaces of both the lateral and medial condyles are concave, particularly centrally. The outer margins of the surfaces are flatter and are the regions in contact with the interarticular discs (menisci) of fibrocartilage in the knee joint.
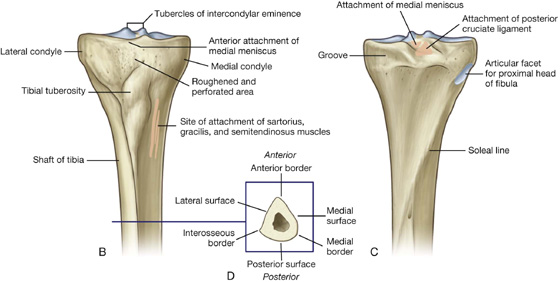
The nonarticular posterior surface of the medial condyle bears a distinct horizontal groove for part of the attachment of the semimembranosus muscle, and the undersurface of the lateral condyle bears a distinct circular facet for articulation with the proximal head of the fibula.
The intercondylar region of the tibial plateau lies between the articular surfaces of the medial and lateral condyles (Fig. 6.37). It is narrow centrally where it is raised to form the intercondylar eminence, the sides of which are elevated further to form medial and lateral intercondylar tubercles.
The intercondylar region bears six distinct facets (Fig. 6.37A) for the attachment of menisci and cruciate ligaments. In addition to these facets, a large anterolateral region of the anterior intercondylar area is roughened and perforated by numerous small nutrient foramina for blood vessels. This region is continuous with a similar surface on the front of the tibia above the tuberosity and lies against infrapatellar connective tissue.
Tibial tuberosity
The tibial tuberosity is a palpable inverted triangular area on the anterior aspect of the tibia below the site of junction between the two condyles (Fig. 6.37A, B). It is the site of attachment for the patellar ligament, which is a continuation of the quadriceps femoris tendon below the patella.
Shaft of tibia
The shaft of the tibia is triangular in cross-section and has three surfaces (posterior, medial, and lateral) and three borders (anterior, interosseous, and medial) (Fig. 6.37D):
 The anterior border is sharp and descends from the tibial tuberosity, where it is continuous superiorly with a ridge that passes along the lateral margin of the tuberosity and onto the lateral condyle.
The anterior border is sharp and descends from the tibial tuberosity, where it is continuous superiorly with a ridge that passes along the lateral margin of the tuberosity and onto the lateral condyle. The interosseous border is a subtle vertical ridge that descends along the lateral aspect of the tibia from the region of bone anterior and inferior to the articular facet for the head of the fibula.
The interosseous border is a subtle vertical ridge that descends along the lateral aspect of the tibia from the region of bone anterior and inferior to the articular facet for the head of the fibula. The medial border is indistinct superiorly, where it begins at the anterior end of the groove on the posterior surface of the medial tibial condyle, but is sharp in the midshaft.
The medial border is indistinct superiorly, where it begins at the anterior end of the groove on the posterior surface of the medial tibial condyle, but is sharp in the midshaft.The large medial surface
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


