Lipoma Gross Specimen This lipoma is surrounded by a thin, delicate, and transparent capsule , and is highly lobulated. It is often taken out by the surgeon piecemeal.
Lipoma, Cut Surface The cut surface of a lipoma is yellow, homogeneous, and greasy. Note the thin, delicate fibrous septa , which separate the tumor into lobules. Some variants may show myxoid areas or small foci of hemorrhage.
Lipoma Showing Abundant Mature Adipose Tissue A conventional lipoma is composed of lobules and sheets of mature adipocytes (white fat). Small- to medium-sized vessels are often scattered in the background but are usually not prominent.
Mature Adipose Tissue The mature adipocytes of a lipoma usually vary little in size from one another. Thin fibrous septa are commonly seen separating the lobules; however, thicker, more fibrotic septa may be present along with fat necrosis in traumatized tumors.
TERMINOLOGY
Definitions
• Benign neoplasm of mature adipocytes (white fat)
CLINICAL ISSUES
Epidemiology
• Incidence
Very common (most common soft tissue tumor overall)
More common in obese people
• Age
Wide range (40-60 yr most common)
Rare in patients < 20 yr old
Site
• Superficial lipomas are most common in upper back, shoulder, neck, and abdomen
Rare in hands, feet, lower legs, and face
• Deep lipomas may arise in deep soft tissues as well as thorax, mediastinum, pelvis, and, rarely, retroperitoneum
May also occur near bone (periosteal/parosteal lipoma)
• Intramuscular lipoma is most common within large muscles of thigh, upper arm, and shoulder
• Mature adipose tissue proliferation within synovium of large joint (synovial lipoma or lipoma arborescens) may clinically simulate diffuse-type tenosynovial giant cell tumor/pigmented villonodular synovitis
Presentation
• Painless mass
Larger lesions may be painful
• May be multiple (5% of cases)
Range in number from several to hundreds
Predilection for upper arm, shoulder, and back in older men
May be hereditary in 30% of cases (familial multiple lipomas)
Multiple lipomas can occur in various syndromes including Cowden, Proteus, and Fröhlich
Treatment
• Surgical excision is curative
Prognosis
• Recurrences are rare
• Higher recurrence rate in intramuscular lipoma (15%)
Clinical Variants
• Lipomatosis
Diffuse &/or regional overgrowth of mature adipose tissue
– Not the same as multiple discrete lipomas
Subtypes: Diffuse, symmetric, pelvic, steroid, and HIV-associated lipodystrophy
Adipose tissue proliferation is poorly marginated, lending tendency toward recurrence
Significant growth may lead to obstruction of regional structures (larynx, ureter, bowel, etc.)
Cytologically and morphologically similar to conventional lipoma, except may show infiltration of muscle or regional structures
MACROSCOPIC
General Features
• Well circumscribed, often lobulated
• Thin, delicate capsule
• Yellow, greasy cut surface
• Myxoid change, focal hemorrhages, bone, or cartilage may be evident
• Infiltrative margins may be present in intramuscular cases
Size
• Usually 2-10 cm
• Deep and intramuscular lipomas are often larger
MICROSCOPIC
Histologic Features
• Lobules and sheets of mature adipocytes
In small samples, adipocytes are often indistinguishable from normal, nonlesional fat
• Minimal variation in adipocyte size
• Bland nuclei are small and often peripherally flattened
May appear absent
May show small intranuclear vacuoles (Lockhern change)
• Small- to medium-sized vessels sparsely distributed throughout tumor
May be more prominent in atrophic lipomas
Only gold members can continue reading. Log In or Register to continue


 , and is highly lobulated. It is often taken out by the surgeon piecemeal.
, and is highly lobulated. It is often taken out by the surgeon piecemeal.
 , which separate the tumor into lobules. Some variants may show myxoid areas or small foci of hemorrhage.
, which separate the tumor into lobules. Some variants may show myxoid areas or small foci of hemorrhage.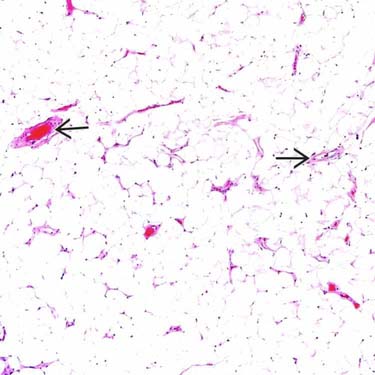
 are often scattered in the background but are usually not prominent.
are often scattered in the background but are usually not prominent.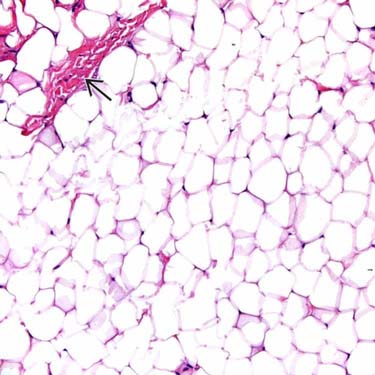
 are commonly seen separating the lobules; however, thicker, more fibrotic septa may be present along with fat necrosis in traumatized tumors.
are commonly seen separating the lobules; however, thicker, more fibrotic septa may be present along with fat necrosis in traumatized tumors.























