Patient Story
A 38-year-old Hispanic woman presents with a rash on her forearms, wrists, ankle, and back (Figures 154-1, 154-2, 154-3, and 154-4). She states the rash is mildly itchy and she does not like the way it looks. She would like some medication to make this better. Lichen planus (LP) was diagnosed and clobetasol was prescribed to keep the LP under better control.
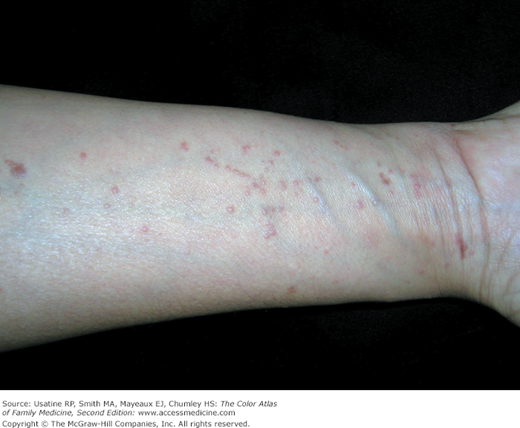

Figure 154-3

Ankle of the woman in Figure 154-1 with typical lichen planus eruption. (Courtesy of Richard P. Usatine, MD.)
Figure 154-4


A. Lichen planus on the back of the woman in Figure 154-1. B. Close-up of lesions on the back showing Wickham striae crossing the flat papules of lichen planus. These lines are white and reticular like a net. (Courtesy of Richard P. Usatine, MD.)
Introduction
Epidemiology
Etiology and Pathophysiology
- Usually idiopathic, thought to be a cell-mediated immune response to an unknown antigen.2,3,5
- Possible human leukocyte antigen (HLA)-associated genetic predisposition.2
- Lichenoid-type reactions may be associated with medications (e.g., angiotensin-converting enzyme inhibitors [ACEIs], thiazide-type diuretics, tetracycline, chloroquine), metals (e.g., gold, mercury), or infections (e.g., secondary syphilis).2,5
- Associated with liver disease, especially related to hepatitis C virus.2,5,6
- LP may be found with other diseases of altered immunity (e.g., ulcerative colitis, alopecia areata, myasthenia gravis).1
- Malignant transformation has been reported in ulcerative oral lesions in men.1
Risk Factors
- Possible HLA-associated genetic predisposition.
- Hepatitis C virus infection, although causal relationship is not established.6
- Certain drugs (see “Etiology and Pathophysiology”).
Diagnosis
- Classically, the six Ps of LP are planar, purple, polygonal, pruritic, papules, and plaques (Figures 154-1, 154-2, 154-3, 154-4, and 154-5).2,5
- These well-demarcated flat-topped violaceous lesions are often covered by lacy, reticular white lines (called Wickham striae or Wickham lines) (Figure 154-4B).
- An initial lesion is usually located on the flexor surface of the limbs, such as the wrists, followed by a generalized eruption with maximal spreading within 2 to 16 weeks.1
- Lesions may demonstrate the Koebner phenomenon (linear distribution) from scratching (Figure 154-2).
- Lesions are more often hyperpigmented rather than purple or pink in dark-skinned persons, and skin may remain hyperpigmented after lesions resolve (Figures 154-6 and 154-7).
- Skin variants
- Hypertrophic—Typical papules develop into thicker reddish-brown to purple plaques (Figures 154-5 and 154-7) most commonly on the foot and shins. Seen more often in black men with hyperpigmented and hypertrophic lesions (Figure 154-7).
- Follicular—Pinpoint hyperkeratotic projections often on scalp, may lead to cicatricial alopecia.
- Vesicular—Vesicles or bullae occur alongside the more typical LP lesions (Figure 154-8).
- Actinic—Typical lesions in sun-exposed areas, such as the face, back of hands and arms (Figure 154-9).
- Atrophic—the lesions are atrophic rather than standard plaques (Figure 154-10).
- Ulcerative—Ulcers develop within typical lesions or start as waxy semitranslucent plaques on palms and soles; may require skin grafting.
- Hypertrophic—Typical papules develop into thicker reddish-brown to purple plaques (Figures 154-5 and 154-7) most commonly on the foot and shins. Seen more often in black men with hyperpigmented and hypertrophic lesions (Figure 154-7).
- Mucous membrane variants
- May be reticular (net-like; Figure 154-11), atrophic, erosive (Figures 154-12 and 154-13), or bullous. It is almost always bilateral.
- Oral lesions may be asymptomatic or have a burning sensation; pain occurs with ulceration.1,4,6
- Oral LP is often associated with extraoral LP.7,8
- May be reticular (net-like; Figure 154-11), atrophic, erosive (Figures 154-12 and 154-13), or bullous. It is almost always bilateral.
- Genitalia variants
- Reticular, annular (Figure 154-14), papular (Figure 154-15), or erosive lesions on penis, scrotum, labia, or vagina.
- Vulvar/vaginal lesions may be associated with dyspareunia, a burning sensation, and/or pruritus.1,7
- Vulvar and urethral stenosis can also be present.1,7
- Reticular, annular (Figure 154-14), papular (Figure 154-15), or erosive lesions on penis, scrotum, labia, or vagina.
- Hair and nail variants; the latter present in 10% of patients.1
- Violaceous, scaly, pruritic papules on the scalp can progress to scarring alopecia. Lichen planopilaris (LP of the scalp) can cause widespread hair loss (see Chapter 189, Scarring Alopecia).9
- Nail plate thinning results in longitudinal grooving and ridging; rarely destruction of nailfold and nail bed with splintering (Figure 154-16).
- Hyperpigmentation, subungual hyperkeratosis, onycholysis, and longitudinal melanonychia can result from LP.1
- Violaceous, scaly, pruritic papules on the scalp can progress to scarring alopecia. Lichen planopilaris (LP of the scalp) can cause widespread hair loss (see Chapter 189, Scarring Alopecia).9






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


