Evidence of genetic studies favors neoplastic process

Likely from bone marrow-derived myeloid dendritic precursors
Clinical Issues
•
Affects infants and children, rarely adults
•
Unisystem disease most often involves bone followed by skin, lymph node, and lung
•
Multisystem disease is subdivided into low and high risk according to involvement of “risk” organs

High-risk organs: Liver, spleen, bone marrow

Liver involvement: 10-15%

Involvement of high-risk organs is associated with poorer prognosis
Microscopic
•
Infiltration of portal tracts and lobules by Langerhans cells

May form small granulomatous nodules or large mass-like lesions

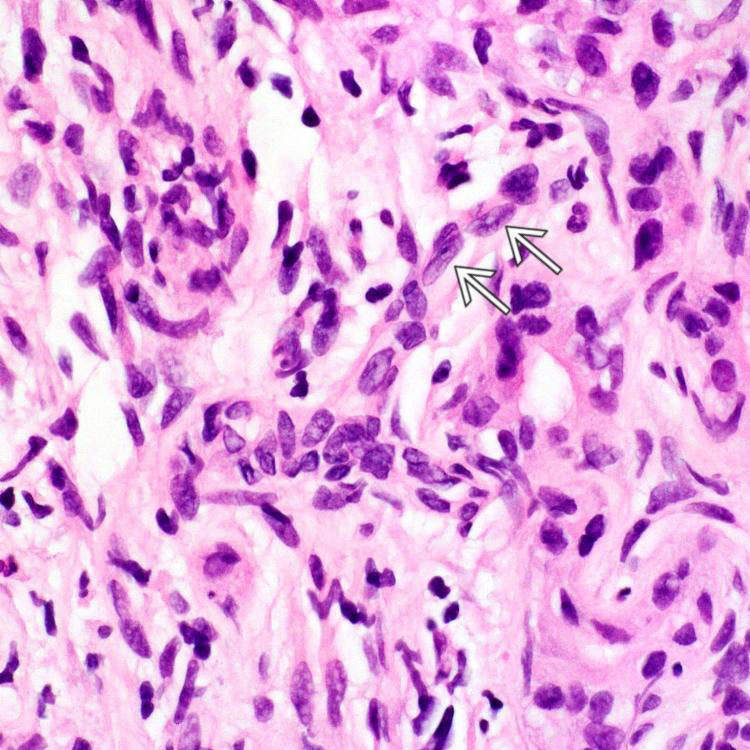
Langerhans cells typically show irregular and elongated nuclei, prominent nuclear grooves and folds, fine chromatin, indistinct nucleoli, abundant pink cytoplasm

Often accompanied by varying numbers of eosinophils, lymphocytes, neutrophils, plasma cells, non-Langerhans histiocytes
•
Bile duct infiltration and destruction

Displacement or replacement of duct epithelial cells by Langerhans cells

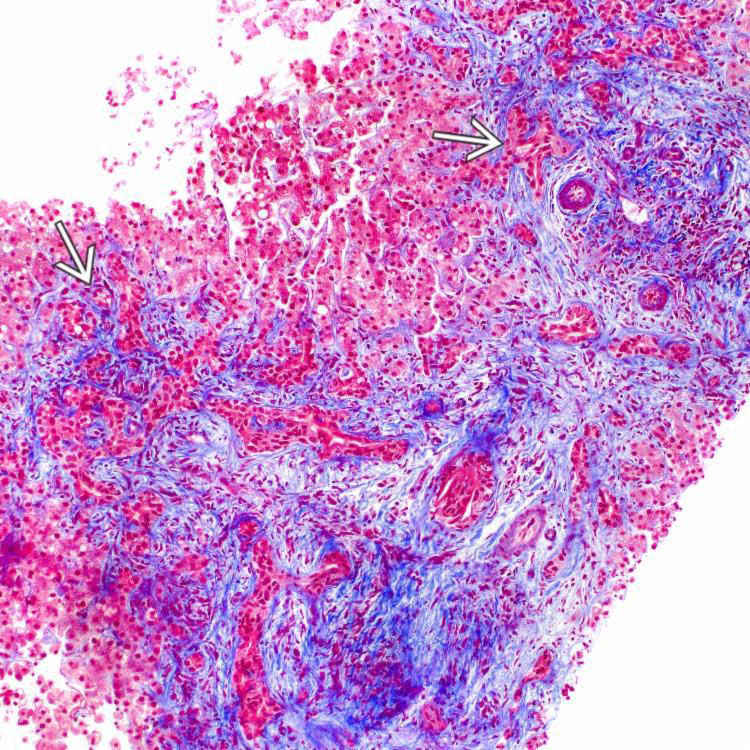
Portal, periportal and periduct concentric fibrosis, duct loss, ductular reaction

May progress to biliary cirrhosis
Ancillary Tests
•
Langerhans cells stain with S100, CD1a, langerin (CD207)
TERMINOLOGY
Abbreviations
•
Langerhans cell histiocytosis (LCH)
Synonyms
•
Eosinophilic granuloma (unifocal LCH)
•
Hans-Schüller-Christian disease (multifocal unisystem LCH)
•
Letterer-Siwe disease (multifocal multisystem LCH)
Definitions
•
Infiltration of liver by proliferating Langerhans cells
ETIOLOGY/PATHOGENESIS
Clonal Proliferation
•
Evidence of genetic studies favors neoplastic process
 BRAF
BRAF V600E mutations seen in 25-64% of cases
 MAP2K1
MAP2K1 mutations seen in 27.5% of cases
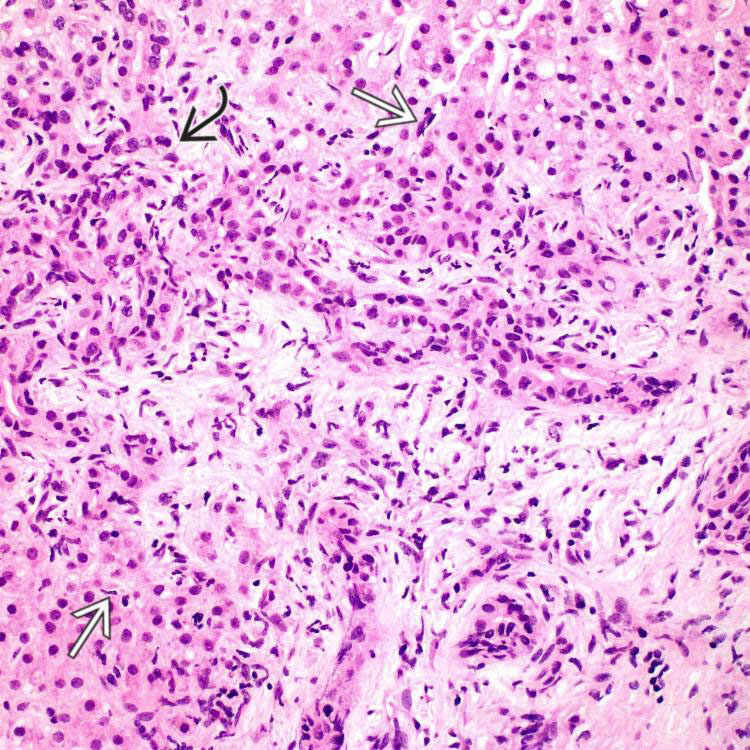
 . Ductular reaction is evident
. Ductular reaction is evident  .
.
 . Scattered lymphocytes and rare neutrophils are seen in this portal tract.
. Scattered lymphocytes and rare neutrophils are seen in this portal tract.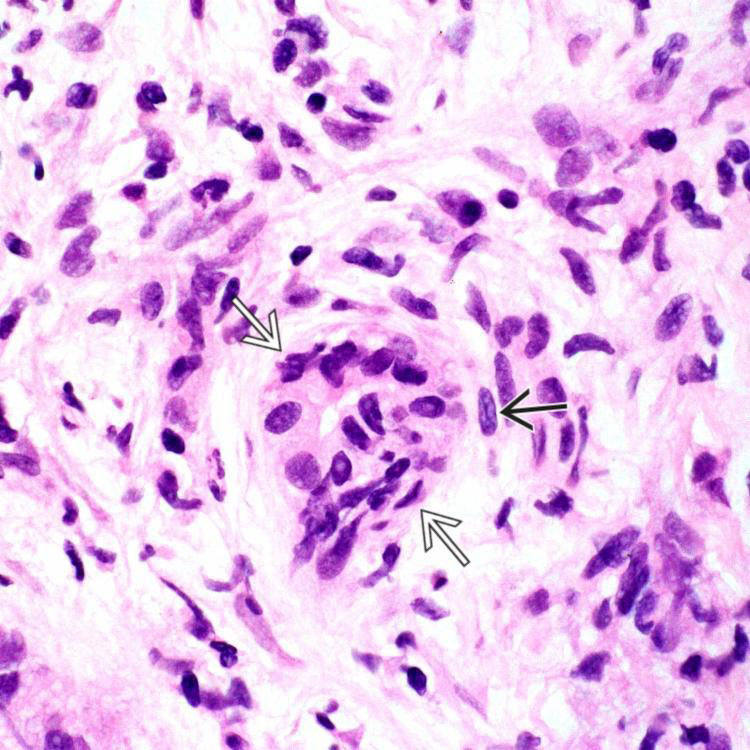
 . Langerhans cells also infiltrate ductules (not shown in this field). Nuclear grooves are noted in some cells
. Langerhans cells also infiltrate ductules (not shown in this field). Nuclear grooves are noted in some cells  .
.
 .
.


