© Teri Shors.
“Where observation is concerned, chance favors only the prepared mind.”
—Louis Pasteur, French chemist and microbiologist (1822–1895)
How do virologists determine which viruses are causing a particular syndrome? If some viral diseases are clinically obvious and there are so few antivirals available to combat them, why are definitive laboratory diagnostic tests developed? Such tests are developed for several reasons:
Patient management is determined by diagnosis. For example, a delivery of a baby by cesarean section may be prudent if a pregnant woman is infected with human immunodeficiency virus (HIV) or has genital herpes or warts at the time of delivery.
Some antiviral therapies are available to treat viral infections. In particular, chemotherapeutic agents are available to treat herpesvirus, influenza A, hepatitis B and C, and HIV infections.
Rapid advancements in the development of antiviral drugs are expanding the range of viral diseases for which a precise diagnosis will become necessary; for example, it was announced in The Lancet (December 12, 2003) that scientists at the U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID) were able to treat rhesus macaques with an experimental drug called recombinant nematode anticoagulant protein c2 (rNAPc2) after the macaques were given a high-dose lethal injection of Ebola virus. To date, there is no cure for Ebola virus disease, but this experimental drug could become an accepted treatment (FIGURE 7-1). On September 14, 2014, positive results were issued in a press release announcing Phase II clinical trials for the use of rNAPc2 as an anticoagulant for the prevention of deep vein thrombosis.
The worst Ebola outbreak in human history started in Guinea in March 2014. More than 11,300 people died, including over 500 healthcare workers. Patrick Sawyer, a consultant for the Liberian finance ministry, collapsed and later died from Ebola virus disease (EVD) after flying on a commercial airplane to Lagos, Nigeria, on July 23, 2014. Despite medical support such as hydration and pain medication, the mortality rate remains at 60% with this particular strain of Ebola virus. Currently, no postexposure treatments for Ebola infection for human use have been approved by the U.S. Food and Drug Administration (FDA). It is paramount that effective therapeutic agents be developed to treat advanced Ebola virus infections.
New drugs under investigation to treat Ebola virus infection include favipiravir, also known as T-105. To date, experiments led by Oestereich and colleagues (a 2014 study published in Antiviral Research) found that T-105 suppressed replication of the Zaire strain of Ebola virus in cell culture. They also performed a small animal study to evaluate the therapeutic efficacy of T-105. Mice infected with the Zaire strain of Ebola virus and treated 6 days after infection with T-105 survived the infection. These results generate cautious optimism that T-105 studies can be continued in a more realistic model system, such as nonhuman primates, and eventually clinical practice.

FIGURE 7-1 (a) Right arm of rhesus monkey treated with rNAPc2 10 days after Ebola infection. The monkey survived. (b) Right arm of untreated rhesus monkey 13 days after infection with Ebola virus. The monkey did not survive.
Other drugs in development include BCX4430, siRNAs, and PMOplus (AVI-7288) and antibody-based approaches such as ZMab, MB-003, and ZMapp, an improved version of MB-003 used to treat two American doctors infected with EVD while taking care of Ebola patients in Liberia during the 2014 outbreak. All but ZMapp are in Phase I or Phase II clinical trials at the time of this writing.
At least seven different vaccine candidates have shown potential to protect nonhuman primates from lethal challenges with Ebola or Marburg viruses. However, the vaccines have not been able to completely protect non-human primates challenged with new (emerging) strains of Ebola virus. Vaccination with a combination of two different genetically modified live attenuated vesicular stomatitis viruses (VSVs) containing the surface glycoprotein from Marburg or Ebola virus (Sudan strain) in place of the VSV glycoprotein have been reported to be protective in rhesus macaques against an emerging strain of Bundibugyo Ebola virus.
Viral infections may demand public health measures to prevent spread to others for several reasons, such as the following:
Blood donors may be asymptomatic carriers of viruses. This is why screening blood banks for HIV, hepatitis B and C viruses, and West Nile virus reduces their spread by blood transfusion.
Documenting novel strains of influenza A virus allows officials to publicly announce health measures that can be implemented, such as the vacci-nation of vulnerable members of the community, including children and the elderly.
The positive identification of viral diseases (such as West Nile encephalitis or yellow fever) linked to mosquito (vectorborne) transmission enables authorities to initiate mosquito-control measures. The introduction of exotic or newly emerging infectious diseases, such as the monkeypox outbreak in the United States in 2003 or hantavirus outbreaks in the United States in Yosemite National Park (2012) and the Texas Panhandle and South Plains (2014), demanded containment, surveillance, and other control measures.
Continuous surveillance of viral infections in the community enables officials to establish means of controlling, monitoring, and evaluating immunization programs. It provides the evidence for new epidemics and new virus–disease associations. It is interesting to note that 90% of all viral diseases were completely unknown at the end of World War II (1945).
This chapter focuses on laboratory diagnosis of viral infections and working with viruses in a research setting. Technology has changed the clinical diagnostic laboratory since the 1990s. Implementing molecular technology is now routine in the form of commercialized kits that give rapid and reliable results.
7.1 Proving Causation of Viral Diseases
Robert Koch, a German physician investigating the causes of anthrax and tuberculosis in cattle during the 1880s, came up with a series of requirements, or postulates, to prove that these diseases were caused by different types of bacterial infections. The four criteria to prove that a specific microbe causes a disease became known as Koch’s postulates:
The microbe must always be associated with every case of the disease, but not with healthy hosts.
The microbe must be isolated from the diseased host and grown in pure culture.
Upon inoculation of the cultured microbe into a healthy host, the same disease is reproduced.
The microbe can be reisolated from the intentionally infected host.
Koch’s postulates worked well to identify bacterial diseases that caused obvious clinical signs and symptoms and could be reproduced in animals experimentally. The requirements reflected the techniques of the 19th century, at a time when bacteriology was in its infancy. Even during Koch’s time, it was realized that fulfillment of the postulates could not be used to demonstrate causality in all cases. There are many exceptions. For example, asymptomatic carriers can host the bacteria that cause typhoid fever and cholera. That is, not all individuals (or animals experimentally) exposed to the pathogenic bacterium that causes tuberculosis will be infected. The discovery of other pathogens, especially viruses, made fulfilling Koch’s postulates more difficult.
Many viral infections are correlated with an asymptomatic carrier state or subclinical infection, such as those caused by HIV, hepatitis C virus, herpes simplex viruses, polioviruses, and West Nile virus. It is known that a very small percentage of individuals who are infected with polioviruses will be paralyzed, yet the polio vaccine that prevents poliovirus infection demonstrates that poliovirus is the causative agent of poliomyelitis. Therefore, Koch’s postulates could not be applied rigidly to every disease.
In the 1930s, Thomas Rivers, an animal virologist, pointed out the limitations of Koch’s postulates for viruses and modified them to prove that viruses caused nonbacterial meningitis in two patients at the Hospital of the Rockefeller Institute for Medical Research. He published a series of papers describing his identification of the etiological agent.
Rivers isolated viruses from the spinal fluid of the patients. His experimentation included the inability to culture a bacterial agent from the patients, filterability of the virus-like agent, and the presence of protective antibodies in the serum from mice and guinea pigs inoculated with the filterable virus-like agent. He formulated the following six criteria that had to be met to prove that a virus caused a particular disease:
Isolation of virus from diseased hosts.
Cultivation of virus in host cells.
Proof of filterability (to exclude larger pathogens).
Production of a comparable disease when the cultivated virus is used to infect experimental animals from the same species as the original host or in related ones.
Reisolation of the same virus from the infected experimental host.
Detection of a specific immune response to the virus.
The biotechnology revolution is enabling rapid advances in medicine. Biotechnology has been especially useful in discovering pathogens that cannot be propagated in pure culture. During the 1990s, Fredricks and Relman modified Koch’s and Rivers’s criteria to reflect the application of new technologies. They proposed criteria for nucleic acid–based evidence of a pathogen using polymerase chain reaction (PCR); (see Refresher: PCR) that must be fulfilled to prove causation. They offer the following guidelines to establish the relationship between a disease and a causative agent:
A nucleic acid sequence of the pathogen should be present in all cases of infectious disease. The microbial nucleic acids should be detected in diseased organs and not in unaffected organs.
No pathogen-associated nucleic acid sequences should be present in healthy hosts or tissues.
After resolution of disease, nucleic acid sequences of the pathogen should no longer be detected. However, if there is a disease relapse, the opposite should occur.
The nucleic acid sequence copy number that correlates with the severity of disease is more likely to be the cause of the disease.
The clinical features and pathologies observed are consistent with the biological properties of the suspected pathogen.
The pathogen or its antigens can be detected in diseased tissue that contains the nucleic acid sequences of the suspected pathogen.
The sequence-based evidence of the pathogen should be reproducible.
Changing technology makes it possible to update Koch’s postulates for defining a causal relationship between a microbe and a disease. The ability to detect nucleic acid sequences in microbes is a powerful tool for identifying previously undiscovered viral and microbial pathogens.
7.2 Viral Diagnostics in the Clinical Laboratory
Over 60% of all infectious disease cases seen by physicians are caused by viruses. Accurate and rapid detection and diagnosis are essential for successful antiviral treatment. In addition to a patient’s travel history, symptoms, and the season of the year, the clinical microbiology laboratory plays an important role in the diagnosis and control of viral diseases.
The type and quality of the specimen collected from the patient and its transportation from the patient to the laboratory limit the ability of the laboratory personnel to perform diagnostic tests. Some diagnostic tests require the virus to be isolated and grown in cell cultures; therefore, transport conditions must ensure that the virus will be viable. It is critical that the collected specimen is representative of the site of infection. The shorter the time interval between the collection of the specimen and its delivery to the laboratory, the more likely that a virus can be isolated from the clinical specimen.
Storage and Collection of Biological Specimens for Viral Testing
The procedure for collecting specimens for viral diagnosis varies. During a medical examination, the physician makes an educated guess as to the likely virus responsible for the patient’s symptoms. The physician collaborates with a clinical microbiologist who determines the appropriate specimens that will be collected for laboratory testing (FIGURE 7-2). Timing of specimen collection is vital to ensure the correct test result. Viral shedding begins shortly before symptoms appear and then rapidly decreases with infections caused by influenza A virus, rhinovirus, and West Nile virus. In contrast, virus shedding during chronic viral infections (e.g., infections caused by cytomegalovirus, hepatitis C virus, and HIV) is prolonged even when the patient is asymptomatic. Specimens collected with swabs are placed into viral transport medium, whereas liquid specimens such as CSF, blood, and urine are not diluted in viral transport medium. If specimens can be processed immediately, they are stored in the refrigerator at 39.2°–46.4°F (4°–8°C). If a specimen must be kept for retrieval at a later date, it is best to store the samples that potentially contain viruses at –94°F (–70°C) or lower. Storing human and animal viruses at –4°F (–20°C) in frost-free freezers results in rapid loss of infectivity. A guide for specimen collection for viral diagnosis of human infections is provided in TABLE 7-1.
Nearly 50% of all specimens collected are from the respiratory tract, and about 30% of viral infections diagnosed in the clinical laboratory are related to respiratory infections. Herpes simplex viruses (cause of oral and genital herpes) and varicella zoster virus (cause of chick-enpox and shingles) can be cultured on a routine basis from dermal lesions. Detection of viruses from blood specimens represents disseminated, invasive infections that may result in systemic disease. Cytomegalovirus (CMV), HIV, hepatitis C and B viruses, parvovirus B19, and adenoviruses are examples of viruses that can be detected from blood specimens. The new gold standard for diagnosis of CNS disease is molecular diagnostics performed on CSF specimens (refer to Case Study 1 at the beginning of the chapter). In cases of gastroenteritis, feces can be used to identify viruses that cannot be grown in cell cultures. Mumps virus, CMV, and adenoviruses are commonly cultured from urine. Conjunctival swabs or corneal scrapings are used to identify corneal eye infections. Herpes simplex viruses and adenoviruses are the most common ocular viral pathogens. Occasionally lung, liver, spleen, kidney, and brain tissues may be used for molecular testing to identify viral pathogens. The fresh tissue is digested with proteases in the presence of a detergent and the nucleic acid extracted for PCR reactions. PCR technology in the clinical laboratory will continue to impact processing of specimens in the coming years.

FIGURE 7-2 Overview of viral diagnosis.
Table 7-1 Specimen Information for Diagnosis of Human Viral Diseases
| General Disease | Potential Virus | Specimen(s) |
|---|---|---|
| Respiratory (e.g., sore throat, bronchitis, pneumonia, croup) | Influenza viruses A and B, rhinovirus, respiratory syncytial virus (RSV), adenovirus, SARS coronavirus (SARS-CoV), MERS coronavirus (MERS-CoV), hantavirus, metapneumonia virus | Nasopharyngeal aspirates, throat swab, sputum, bronchoalveolar lavage for lower respiratory tract infections |
| Skin rashes (maculopapulara or vesicularb) | Herpes simplex viruses, measles virus, rubella virus, varicella zoster virus, human herpesvirus 6, human herpesvirus 8, monkeypox virus | Swab or aspirate fluid in vesicle and scrape cells at the base of the lesion |
| Central nervous system (e.g., aseptic meningitis and encephalitis) | Herpes simplex virus, cytomegalovirus (CMV), coxsackie virus A, enterovirus, rabies virus, varicella zoster virus, dengue virus, chikungunya virus, West Nile virus | Cerebrospinal fluid, brain tissue; blood for some insectborne viruses like dengue and chikungunya virus |
| Hepatitis | Hepatitis A, B, and C viruses | Serum |
| Congenital infections | CMV, herpes simplex virus | Serum, urine (for CMV), amniotic fluid |
| Genital infections | Papillomaviruses, herpes simplex viruses | Genital or vesicle swab, vesicle scrapings, endocervical swab and biopsy tissue (for papillomaviruses) |
| Infectious mononucleosis | Epstein-Barr virus, CMV | Blood, plasma, peripheral blood lymphocytes |
| Eye infections | Herpes simplex virus, adenovirus | Corneal scraping, dermal swab, throat swab, eye swab |
| Immunodeficiency | Human immunodeficiency virus types 1 and 2 (HIV-1 and HIV-2) | Blood, plasma |
The Five General Approaches for Laboratory Diagnosis of Viral Infections
Similar to detection and identification methods for bacteria, five approaches for laboratory diagnosis of viral infections are used:
Microscopy
Viral antigen detection
Culture
Nucleic acid detection
Antibody detection
TABLE 7-2 lists detection approaches used to routinely detect human viruses in the clinical virology laboratory.
Microscopy
Microscopic detection of viruses has taken two directions: (1) light microscopy to observe intracellular inclusions, or clumps of viruses within cells, and (2) electron microscopy to observe individual virus particles. Light microscopic examination of stained histo-logical tissues or lesions for viral inclusions is a rapid test used for such viruses as measles, herpes simplex, and varicella zoster. For more than 60 years, immunofluorescence has been one of the primary technologies used by diagnostic virology laboratories. Specimens are fixed and frozen tissues are prepared on slides. Tissue cultures also can be grown on glass slides. Virus-specific antibodies containing a fluorescent tag bound to the Fc region of the antibody are allowed to react with the specimen. Antibodies are proteins produced by the host in response to a particular pathogen (see Refresher: Immunology Terms). fluorescent antibodies are used as a stain to detect specific viral antigens present in the clinical specimen or virus-infected cell cultures. Any unbound antibody is washed away and the specimen is observed with a fluorescent microscope. Fluorescent microscopes have the same resolving power as light microscopes. Immunofluorescence relies on differential cytopathic effects for virus detection (refer to Section 7.4, “Working with Viruses in the Research Laboratory”). FIGURE 7-3 shows the detection of Epstein-Barr viral antigens using indirect immunofluorescence. An application of this method that has more limited use is immunohistochemistry (IHC). The advantage of IHC is that viral antigens can be detected in the absence of well-defined viral inclusions. It, too, uses antibodies to localize viral proteins in fixed tissue sections or cell cultures.
Table 7-2 Detection and Identification of Human Viruses in the Clinical Laboratory*
| Virus | Microscopy | Antigen Detection | Nucleic Acid Detection | Culture | Antibody Detection | Comments |
|---|---|---|---|---|---|---|
| Adenoviruses | 2 | 1 | 1 | 1 | 3 | IFA and culture are often used for respiratory specimens. IHC for tissue specimens. NAATs used to monitor viral load in compromised hosts. |
| Hantaviruses | 3 | 1 | 2 | 3 | 1 | BSL-4 lab needed for culture. Serology and NAATs in specialized labs useful for diagnosis. IHC used in fatal cases. |
| Influenza A and B viruses | 3 | 1 | 1 | 1 | 2 | Rapid antigen tests widely used but not optimal in sensitivity and specificity. NAAT is most sensitive but not widely used. Serology is used for epidemiological or retrospective studies. |
| Coronaviruses | 3 | 1 | 3 | 3 | 2 | NAATs and antibody tests for SARS-CoV must be confirmed by reference laboratory. |
| Parainfluenza viruses | 1 | 2 | 1 | 1 | 3 | IFA is the most widely accepted detection method. |
| Rhinoviruses | 3 | 2 | 3 | 1 | 3 | Most common testing in the clinical laboratory is culturing. NAAT is used in epidemiologic studies and research. |
| Respiratory syncytial virus (RSV) | 2 | 1 | 1 | 1 | 3 | Rapid antigen tests, especially IFA most widely used. |
| Human metapneumonovirus | 3 | 1 | 3 | 2 | 3 | NAAT is the main diagnostic method. Conventional culture is difficult. |
| Noroviruses | 2 | 2 | 3 | 3 | 3 | EM used in equipped laboratory. NAAT is challenging due to strain variability. |
| Rotaviruses | 2 | 2 | 1 | 3 | 3 | Direct antigen detection is the top choice for diagnosis. EM useful if available. |
| Other enteroviruses | 3 | 1 | 1 | 1 | 3 | Enterovirus RNA detection used for central nervous system infections. |
| Epstein-Barr virus | 3 | 1 | 2 | 3 | 1 | Serology is used routinely. NAATs used for viral-related tumors. IHC or ISH used on tumor biopsy specimens. |
| Papillomaviruses | 3 | 1 | 3 | 3 | 3 | NAAT is used for detection and genotype differentiation. Human immunodeficiency virus |
| Human immunodeficiency virus | 3 | 2 | 1 | 3 | 1 | Serology is the primary diagnostic method. Proviral DNA and plasma RNA levels are used to monitor viral load to guide therapy. |
| Hepatitis C and G viruses | 3 | 1 | 3 | 3 | 1 | Serology is used for diagnosis. NAATs are used to monitor viral load in response to therapy. |
| Human T cell lymphotropic virus | 3 | 2 | 3 | 3 | 1 | Serology is the test for diagnosis. NAAT is useful for virus identification in HTLV. |
| Hepatitis A virus | 3 | 3 | 3 | 3 | 1 | Serology is the standard diagnostic test. |
| Hepatitis B virus | 3 | 1 | 1 | 3 | 1 | Viral antigens and antibodies as well as NAATs are used for monitoring the course of infection and therapy. |
| Hepatitis D virus | 3 | 2 | 2 | 3 | 3 | Testing only done by reference laboratories. Diagnosis is only used if patient also has hepatitis B infection. IHC of biopsy tissue is useful for diagnosis. |
| Hepatitis E virus | 3 | 2 | 3 | 3 | 1 | Serology is the standard diagnostic test. |
| Herpes simplex virus | 2 | 1 | 1 | 1 | 2 | Shell vial is used for rapid determination of viral replication. IFA and IHC used for rapid detection in skin or mucous membrane lesions. NAAT is used for central nervous system infections. |
| Varicella zoster virus | 1 | 1 | 1 | 1 | 2 | IFA and NAATs are commonly used as rapid tests. |
| Cytomegaloviruses | 2 | 1 | 1 | 1 | 2 | IHC is used on tissue specimens. Serology primarily used to determine prior infection. NAATs used to assess risk of disease and response to therapy. |
| Herpesviruses 6 and 7 | 3 | 1 | 1 | 3 | 2 | NAATs are the choice for diagnostics. |
| Herpesvirus 8 | 3 | 1 | 1 | 3 | 2 | Serology is used to identify infected persons. IHC used to for Kaposi’s sarcomas. |
| Filoviruses and arenaviruses | 1 | 1 | 1 | 1 | 2 | BSL-4 lab needed for culturing. Testing confined to specialized laboratories. Lymphocytic choriomeningitis virus (LCM) diagnosed by serology. |
| Measles virus | 2 | 3 | 2 | 2 | 1 | Serology is most useful for diagnosis and determination of immunity. |
| Mumps virus | 2 | 3 | 3 | 1 | 1 | |
| Rubella virus | 3 | 2 | 3 | 1 | 1 | |
| Parvoviruses | 3 | 1 | 3 | 3 | 1 | |
| Arboviruses | 3 | 2 | 3 | 3 | 1 | |
| Hendra and Nipah viruses | 3 | 1 | 2 | 2 | 1 | |
| Rabies virus | 2 | 2 | 1 | 2 | 2 | |
| Poxviruses | 1 | 1 | 3 | 1 | 1 | |
*Key: 1 = approach is useful for diagnostic purposes; 2 = approach is useful under certain circumstances or for the diagnostics of specific infections; 3 = a test that is seldom useful for diagnostic purposes. Abbreviations: IHC, immunohistochemistry; IFA, immunofluorescence assay; NAAT, nucleic acid amplification assay; ISH, in situ hybridization; EM, electron microscopy; BSL, biosafety level. Information from Mandell, G. G., et al., eds. 2010. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia: Churchill Livingstone Elsevier; Table 17.18, pp. 259–260. | ||||||
Individual virus particles cannot be seen with the light microscope and are considered invisible or ultramicroscopic because of their small size (30–300 nanometers [nm]). The development of electron microscopy, which resolves structures at 0.5 nm, became a rapid way to visualize virus particles in the clinical laboratory; however, few diagnostic laboratories currently use this technique. Electron microscopy is used to directly visualize virus particles present in a clinical specimen. The morphology (shape) of the particle enables an examiner to assign the virus to a particular family of viruses. It is a rapid method (involving a simple and fast negative-staining procedure) that is especially useful for examining viruses that cannot replicate in cell cultures. Application of the electron microscope during the late 1940s involved distinguishing poxviruses such as variola virus (which causes smallpox), monkeypox virus, and molluscum contagiosum virus from varicella zoster virus (a herpesvirus that causes chickenpox). In the 1970s, electron microscopy led to unexpected findings, especially the detection of viruses present in stool specimens from young children suffering from gastroenteritis.

FIGURE 7-3 Rapid diagnosis of Epstein-Barr virus (EBV) infection by indirect immunofluorescent staining of infected cells. Patient serum was collected to determine whether the individual had a primary diagnosis of infection (infectious mononucleosis, IgM EBV antibodies) or reactivation of a latent virus (IgG antibodies).

FIGURE 7-4 A fecal sample was collected from a 1-year-old patient with diarrhea. The images show that multiple agents were observed in the sample. An arrowhead points to adenovirus particles, and an arrow points to incomplete rotavirus particles.
Electron microscopy has limitations, though. For one, it is not a sensitive method. At least 1 to 10 million viruses must be present in 1 milliliter (mL) of the clinical specimen to visualize the virus by electron microscopy. It also requires a skilled microscopist and an expensive electron microscope for examination of samples. Certain clinical specimens, such as feces and mucus, contain high enough concentrations of virus particles that they can be visualized via electron microscopy.
Immunoelectron microscopy is used to concentrate the number of virus particles in a given sample. Antibodies specific to a suspected viral pathogen are added to the specimens. The virus–antibody complexes are concentrated by centrifugation directly onto a specimen grid. Subsequently, the sample is negatively stained and viewed using the electron microscope. FIGURE 7-4 is an electron micrograph of specimens prepared in this manner. The technique can be slightly modified to increase the sensitivity of the assay. Labeling antibody molecules with electron-dense markers such as colloidal gold is used in various protocols to enhance visualization of the virus–antibody reaction. Noroviruses, rotaviruses, coronaviruses, astroviruses, hepatitis A virus, and adenoviruses were identified this way in clinical specimens (FIGURE 7-5).
Detection of Viral Antigens
A large number of commercially available test kits are available for viral antigen detection and are routinely used in clinical laboratories. The tests are inexpensive, technically easy to perform, and permit a rapid turnaround time. Methods that use antigen detection include enzyme-linked immunosorbent assays (ElisAs) and hemagglutination assays (refer to Section 7.4, “Working with Viruses in the Research Laboratory”). For example, respiratory syncytial virus (RSV) and influenza A and B viruses can be detected within an hour of the receipt of a given specimen. These tests are very useful during peak months of transmission.

FIGURE 7-5 Electron micrograph of parvovirus B19 (the causative agent of erythema infectiosum, also known as fifth disease) using immunoelectron microscopy procedure. Virions/immune complexes were centrifuged directly onto a specimen grid. The arrowhead points to a genome-defective virus particle.

FIGURE 7-6 (a) Schematic illustrating the ELISA procedure used to detect antibodies in patient serum. Briefly, patient serum is added to wells (typically 96-well plastic plates) precoated with known viral antigens. If virus-specific antibodies are present, they will bind to the viral antigens. Next, antihuman IgG enzyme-labeled antibodies are added, which react with human antibodies. The enzyme substrate solution is then added. If a color develops, it indicates that the reaction is positive. Note: Rigorous washing follows each incubation step. (b) Schematic illustrating the ELISA procedure used to detect viral antigens present in a clinical sample (e.g., feces, throat, or nasal wash). The clinical sample is added to wells precoated with virus-specific antibodies. If viral antigens are present in the clinical sample, they will bind to the virus-specific antibodies. Next, enzyme-labeled antiviral antibodies are added, followed by substrate solution. If a color develops, it indicates the reaction is positive. Note: Rigorous washing follows each incubation step.
ELISAs are based on antibodies binding to their antigens and the detection of this reaction using a commercial antibody conjugated with an active enzyme. The antibody-tagged enzyme reacts with its substrate to produce a color change. Observing and measuring the color determine the test result. FIGURE 7-6 illustrates the detection of viral antigens present in plasma or serum antibodies in clinical samples. FIGURE 7-7 is a photograph of an ELISA test used to determine whether HIV-1 antibodies were present in a person’s serum. ELISA is a very sensitive method and will result in a reaction even if only one or two antibodies are present in the serum sample.
Laboratory testing recommendations for the diagnosis of HIV infection were updated on June 27, 2014. The Centers for Disease Control and Prevention’s (CDC) modified recommendations were necessary because new FDA-approved HIV immunoassays enable detection of HIV sooner after infection than did previous assays. Confirmation tests that relied on a western blot could produce false-negative or indeterminate results if individuals were in the very early course of HIV infection. For this reason, new procedures were recommended and are illustrated in the flow diagram in FIGURE 7-8. The recommendations are for laboratory personnel on the use of FDA-approved assays for the diagnosis of HIV infection in adults and children older than 2 years of age.

FIGURE 7-7 HIV ELISA test. This 96-well plate is read via a spectrophotometer. The yellow color indicates a positive antigen–antibody reaction. The ELISA test involves adding patient serum to wells coated with lysed HIV-infected T cells. Any anti-HIV antibodies present in patient serum will bind to the viral antigens from the T cells. After a washing step, enzyme-labeled antihuman IgG is added, followed by a chromagenic substrate for the enzyme that when acted upon by the enzyme produces a colored product if anti-HIV antibodies are present.
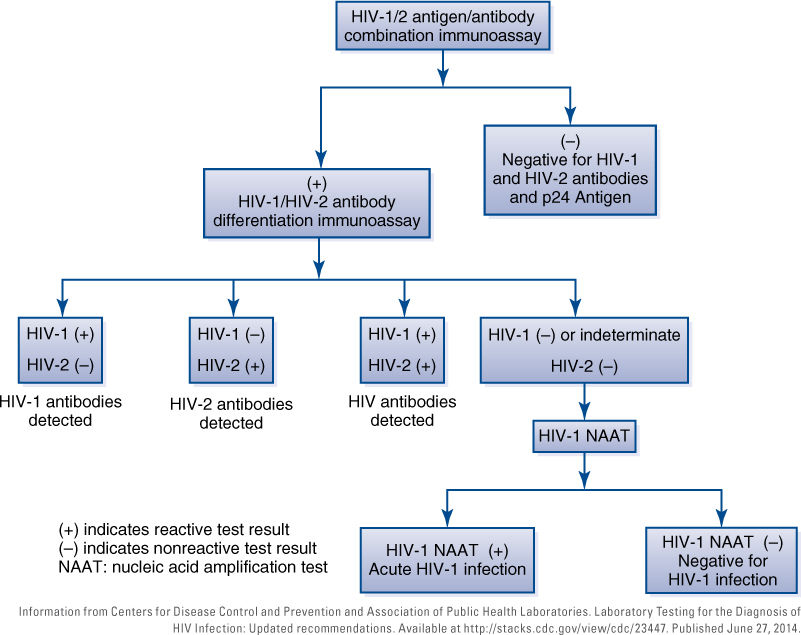
FIGURE 7-8 Flow diagram illustrating the procedural strategy for HIV testing in the United States.
In brief, a combination immunoassay that detects both HIV-1 and HIV-2 antibodies and HIV-1 p24 antigen should be performed on clinical plasma or serum samples. Any samples that react positively should undergo a second testing with an immunoassay that distinguishes HIV-1 from HIV-2 antibodies. Patient samples that are positive in the first immunoassay but nonreactive or indeterminate by the antibody differentiation assay should proceed to HIV nucleic acid testing (NAATs) for final confirmation. The NAATs results will be used to identify persons who are infected, or who are uninfected, and for reporting evidence of HIV infection to public health authorities.
Culture
Viruses require a living host cell for replication. Cell cultures are derived from cells taken from original tissue using enzymatic, mechanical, or chemical processes. The cells are grown in culture medium as monolayers and used for routine virus isolation and identification. Cell cultures were used in research laboratories to study viruses by the early 1960s but were not used in diagnostic laboratories until the early 1970s (see Section 7.4, “Working with Viruses in the Research Laboratory”). No particular cell culture line can support the replication of all viruses, so diagnostic laboratories use multiple cell lines. Cell cultures (TABLE 7-3) permissive to infection by suspected viruses in the clinical specimen are inoculated with the clinical specimen. The inoculated cultures are monitored daily for cytopathic effects (CPEs). CPEs are visual changes in the infected cell culture that are caused by viral replication. The inoculated cultures are monitored for CPEs and compared to uninoculated control cell cultures. After 50% of the monolayer has CPEs, the virus-induced changes can be visualized with an inverted light microscope under low power or the infected cells will be analyzed by other techniques such as PCR or immunofluorescence.
It can take days to weeks for CPEs to occur. Rapid diagnosis is increasingly important in patient management. The centrifugation culture (shell vial technique) is used in clinical labs for rapid diagnosis of viral infections. It allows the laboratory technician to detect viral antigens before CPEs are present in a given clinical specimen. The basic protocol entails adding culture cells grown in suspension to shell vials containing a cover slip on the bottom of the vial, allowing cells to form mono-layers at the bottom of the vial, inoculating with patient specimen (virus), performing a slow-speed centrifugation step (1,000 rpm for about 45 minutes) to increase the infectivity of the virus, incubating the specimen (about 36 hours), and then fixing the monolayers with acetone. Cover slips from the shell vials are stained with fluorescent monoclonal antibodies and examined under a fluorescence microscope (FIGURE 7-9). Some laboratories use a mixture of cell lines such as mink lung cells (strain Mv1Lu) and A549 cells in the same shell vial, which is especially suited for the rapid detection of early viral antigens. Shell vial cultures can be stopped and negative results reported at 2 days, rather than 7–14 days using conventional cell culture methods (TABLE 7-4).
Table 7-3 Cell Lines Commonly Used in Diagnostic Virology Laboratories
| Replication in Cell Cultures | ||||
|---|---|---|---|---|
| Virus | PMK | HDF | Hep-2 | A549 |
| Adenovirus | + | + + | + + + | + + + |
| Cytomegalovirus | – | + + + | – | – |
| Enterovirus | + + + | + + | +/– | +/– |
| Herpes simplex virus | + | + + | + + | + + + |
| Influenza virus | + + + | + | – | – |
| Parainfluenza virus | + + + | + | +/– | +/– |
| Rhinovirus | + | + + + | + | – |
| Varicella zoster virus | + | + + + | – | + + + |
Key: + + + Replicates very well, + + Moderate replication, + Replicates poorly, +/– Variable replication, – No replication. Abbreviations: PMK, primary monkey kidney cell line; HDF, human diploid fibroblasts; HEp-2, human epidermoid larynx carcinoma cell line; A549, human heteroploid lung carcinoma cell line. Information from Clinical Virology Manual, Fourth Edition. S. Specter, R. L. Hodinka, S. A. Young, D. L. Wiedbrauk, Editors, Chapter 3: Primary Isolation of Viruses, p. 37, Table 2. Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| ||||