26
Introduction to Endocrinology: The Hypothalamic–Pituitary Axis
This chapter will be most useful after having a basic understanding of the material in Chapter 38, Introduction to Endocrinology: The Hypothalamic Pituitary Axis in Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 12th Edition. In addition to the material presented here, the 12th Edition includes:
• A detailed discussion of the hypothalamic-pituitary-endocrine axis
• A description of the pituitary hormones and their releasing factors
• A discussion of the therapy of growth hormone (GH) deficiency
• A discussion of the glycoprotein hormones: thyroid stimulating hormone (TSH) and gonadotropins
• A discussion of the posterior pituitary hormones: oxytocin and vasopressin
LEARNING OBJECTIVES
 Understand the functioning of the hypothalamic-pituitary axis.
Understand the functioning of the hypothalamic-pituitary axis.
 Describe the pharmacotherapy of GH excess and GH deficiency.
Describe the pharmacotherapy of GH excess and GH deficiency.
 Develop knowledge of the clinical uses of gonadotropin-releasing hormone (GnRH) and its analogs.
Develop knowledge of the clinical uses of gonadotropin-releasing hormone (GnRH) and its analogs.
DRUGS INCLUDED IN THIS CHAPTER
Bromocriptine (PARLODEL, CYLOSERT, others)
Cabergoline (CABERLIN, DOSTINEX, CABASER)
Cetrorelix (CETROTIDE)
Choriogonadotropin alfa (OVIDREL)
Follitropin α (GONAL-F)
Follitropin β (FOLLISTIM, PUREGON)
Ganirelix (ANTAGON)
Gonadorelin (FACTREL, LUTREPULSE)
Goserelin (ZOLADEX)
Histrelin (VANTAS, SUPPRELIN LA)
Lanreotide (SOMATULINE LA, SOMATULINE DEPOT)
Leuprolide (LUPRON, ELIGARD)
Lutropin alfa (LUVERIS, LHADI)
Mecasermin (INCRELEX)
Menotropins (REPRONEX)
Nafarelin (SYNAREL)
Octreotide (SANDOSTATIN, SANDOSTATIN-LAR DEPOT)
Oxytocin
Pegvisomant (SOMAVERT)
Pergolide (PERMAX)
Quinagolide (NORPROLAC)
Recombinant human growth hormoneGH (ACCRETRTROPIN, GENOTROPIN, HUMATROPE, NORDITROPIN, NUTROPIN, OMNITROPE, SAIZEN, SERPSTIM, TEV-TROPIN, ZORBTIVE, NUTROPINE DEPOT)
Triptorelin (TRELSTAR DEPOT LA)
Urine-derived human chorionic gonadotropin (hCG; NOVAREL, PREGNYL, PROFASI)
Urofollitropin (uFSH; BRAVELLE, MENOPUR)
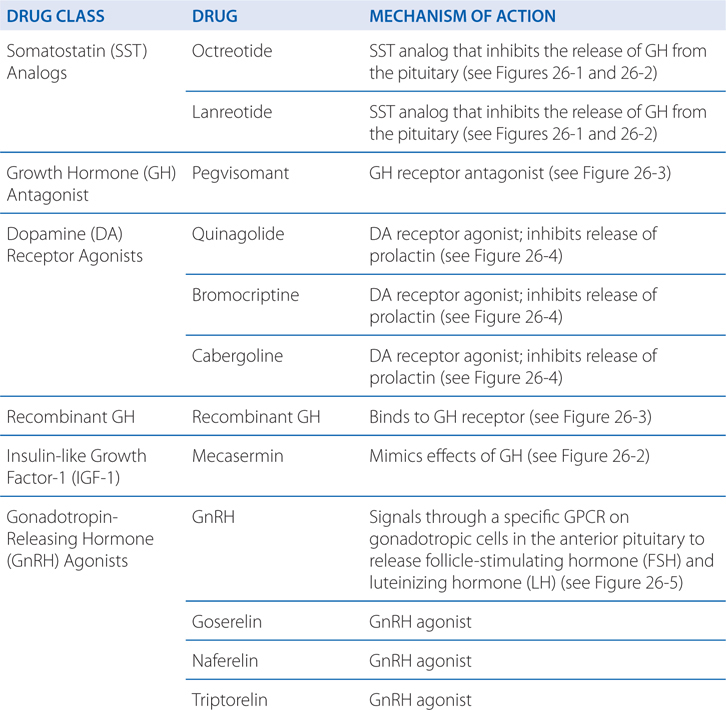
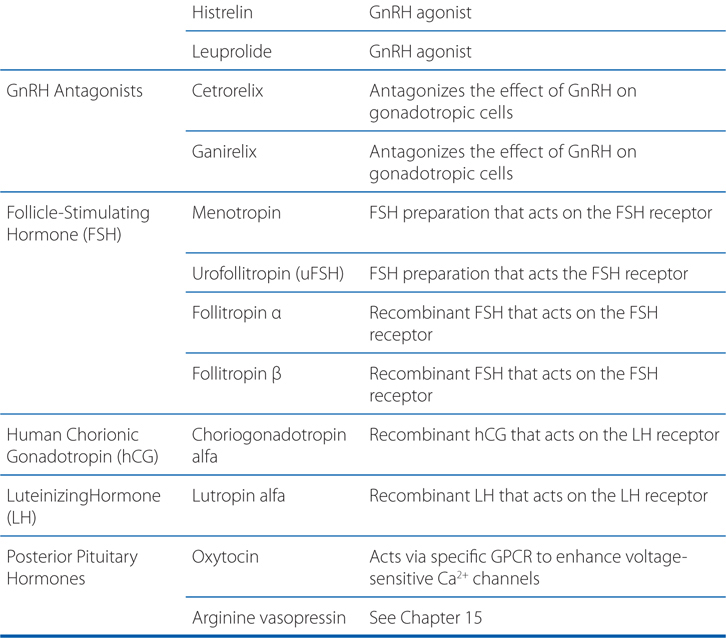
MECHANISMS OF ACTION OF DRUGS THAT ACT ON THE HYPOTHALAMIC-PITUITARY AXIS
A 43-year-old man of normal height has been diagnosed with acromegaly.
a. What is acromegaly and why is this patient’s height normal?
Acromegaly is the result of excess secretion of GH from an anterior pituitary adenoma. The organization of the posterior and anterior pituitary glands is shown in Figure 26-1. In adults, the signs and symptoms of acromegaly are arthropathy, carpal tunnel syndrome, visceromegaly, macroglossia, hypertension, glucose intolerance, headache, lethargy, excess perspiration, and sleep apnea. If the epiphyses are unclosed (presumably the epiphyses are closed in this patient), the GH excess results in increased longitudinal growth and gigantism.
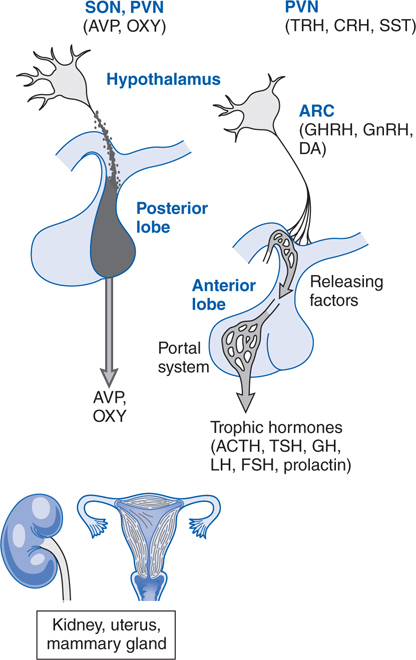
FIGURE 26-1 Organization of the anterior and posterior pituitary gland. Hypothalamic neurons in the supraoptic (SON) and paraventricular (PVN) nuclei synthesize arginine vasopressin (AVP) or oxytocin (OXY). Most of their axons project directly to the posterior pituitary, from which AVP and OXY are secreted into the systemic circulation to regulate their target tissues. Neurons that regulate the anterior lobe cluster in the mediobasal hypothalamus, including the PVN and the arcuate (ARC) nuclei. They secrete hypothalamic-releasing hormones, which reach the anterior pituitary via the hypothalamic-adenohypophyseal portal system and stimulate distinct populations of pituitary cells. These cells, in turn, secrete the trophic (signal) hormones, which regulate endocrine organs and other tissues. ACTH, Adrenocorticotrophic hormone; CRH, corticotropin-releasing hormone; DA, dopamine; FSH, follicle-stimulating hormone; GH, growth hormone; GHRH, growth hormone-releasing hormone; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; TRH, thyrotropin-releasing hormone; TSH, thyroid-stimulating hormone.
b. How is GH secretion regulated?
Growth hormone–releasing hormone (GHRH) and somatostatin (SST), released from the hypothalamus, stimulate or inhibit the release of GH from the pituitary, respectively (see Figure 26-2). Insulin-like growth factor (IGF-1), a product of GH action on peripheral tissues, causes negative feedback inhibition of GH release at the level of the hypothalamus and the pituitary.
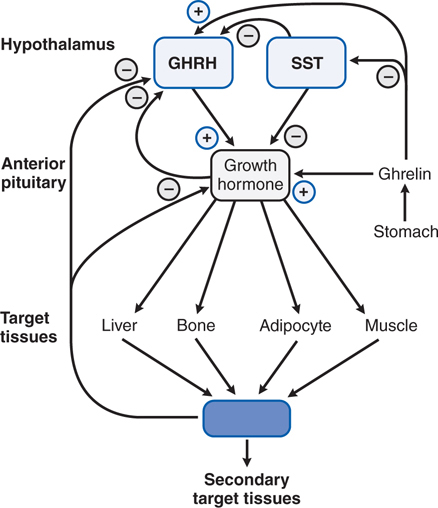
FIGURE 26-2 Growth hormone secretion and actions. Two hypothalamic factors, growth hormone–releasing hormone (GHRH) and somatostatin (SST) stimulate or inhibit the release of growth hormone (GH) from the pituitary, respectively. Insulin-like growth factor-1 (IGF-1), a product of GH action on peripheral tissues, causes negative feedback inhibition of GH release by acting at the hypothalamus and the pituitary. The actions of GH can be direct or indirect (mediated by IGF-1). Inhibition, –; stimulation, +.
c. How does GH cause its myriad of effects on various tissues?
GH and prolactin act on specific receptors in target tissues. The GH receptor is a widely distributed cell surface receptor that consists of an extracellular hormone-binding domain, a single membrane-spanning region, and an intracellular domain that mediates signal transduction (see Figure 26-3).
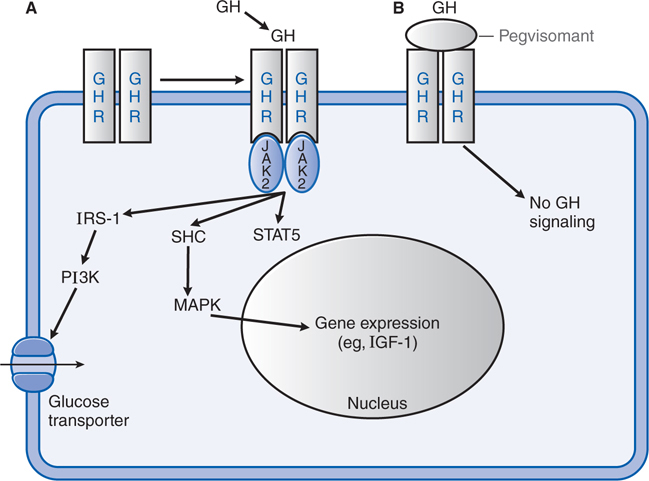
FIGURE 26-3 Mechanisms of growth hormone and prolactin action and of GH receptor antagonism. Left (A):
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


