Most frequent in females, usually younger patients
Better prognosis (3-year survival rate of 56%, systemic variant: 22%)
Microscopic
• IVLBCL cells are large, with vesicular nuclear chromatin, distinct nucleoli, and frequent mitoses
• Lymphoma cells are mainly located in lumina of small vessels
• Mitoses are frequent
• Fibrin thrombi, hemorrhage, and necrosis often seen
• Circulating lymphoma cells can be occasionally seen in peripheral blood
Ancillary Tests
• Pan-B-cell markers (+), Bcl-2(+), MUM1(+)
• Bcl-2(+) (90%), MUM1(+) (95%)
• CD5(+) (30%); other T-cell markers (-)
• Ki-67 high
Top Differential Diagnoses
• Peripheral T- or NK-cell lymphomas with intravascular pattern
• Hepatosplenic T-cell lymphoma
• T-cell large granular lymphocytic leukemia
• Diffuse large B-cell lymphoma, not otherwise specified
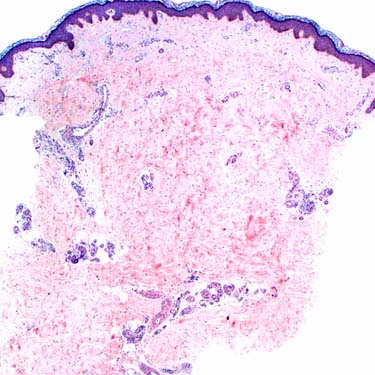
Morphologic Features of IVLBCL Intravascular large B-cell lymphoma (IVLBCL) involving skin is shown. Note that the infiltration by neoplastic cells is difficult to recognize at this low magnification.
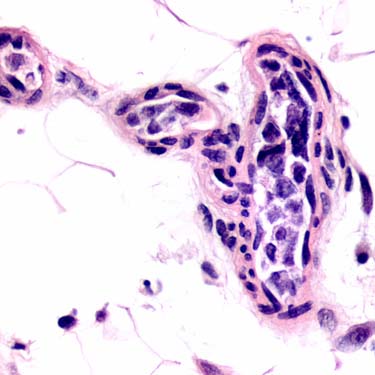
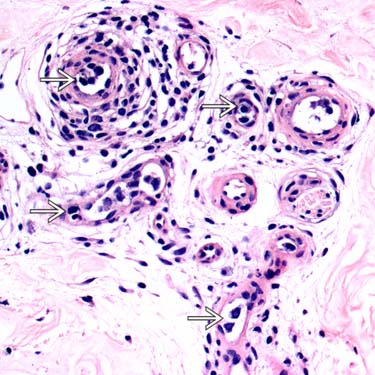
Morphologic Features of IVLBCL IVLBCL involving the skin is shown. At high power, atypical lymphoid cells are seen inside of small dermal vessels .
Morphologic Features of IVLBCL Subcutaneous adipose tissue shows involvement by IVLBCL. Small blood vessels are filled with large atypical neoplastic cells.
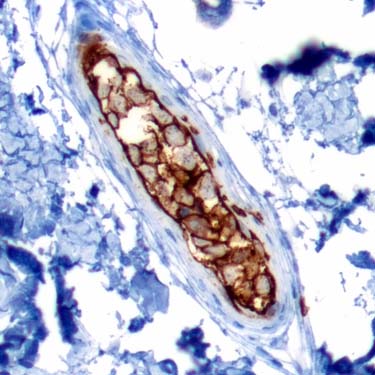
Ancillary Studies (CD20) CD20 highlights the intravascular large neoplastic cells, supporting B-cell lineage and the diagnosis of IVLBCL involving subcutaneous adipose tissue.
TERMINOLOGY
Abbreviations
• Intravascular large B-cell lymphoma (IVLBCL)
Synonyms
• Angiotropic large cell lymphoma
• Angioendotheliotropic (intravascular) lymphoma
• Intravascular lymphomatosis
Definitions
• Large B-cell lymphoma characterized by selective intravascular growth
• Preferential intravascular growth is condition sine qua non for diagnosing IVLBCL
Concomitant and minimal extravascular location of neoplastic cells, usually surrounding involved vessels, can be seen
CLINICAL ISSUES
Site
• Selective tumor growth within lumina of small blood vessels, particularly capillaries
• Widely disseminated
• Any organ can be involved
• Absence of marked lymphadenopathy
• Mechanisms responsible for selective growth of neoplastic cells within blood vessel lumina are unknown; possible explanations include
Chemokine-chemokine receptor interactions
– e.g., CXCL9 (expressed in endothelium) and CXCR3 (expressed in IVLBCL)
Decreased expression of adhesion molecules on surface of IVLBCL cells
– e.g., CD29 and CD54
Presentation
• Middle-aged or elderly patients; median: 67 years
• M:F ratio = 1.3:1
• IVLBCL can involve any organ with heterogeneous, often nonspecific symptoms
Fever of unknown origin
General fatigue
Deterioration in performance status
• Diagnosis can be clinically difficult and some cases are diagnosed postmortem
• 2 major patterns of clinical presentation
Western IVLBCL
– Predominant neurologic and dermatologic manifestations
– Central nervous system is involved in most patients
Asian IVLBCL
– Hemophagocytic syndrome
– Fever and B symptoms
– Pancytopenia and bone marrow infiltration
– Skin and central nervous system involvement are uncommon
• Skin
Heterogeneous clinical presentation
– Nodules/plaques (49%)
– Macules (22.5%)
– Telangiectatic patches (20%)
– Cellulitis
– Ulcerated nodules
Waxing and waning lesions (16%)
Lower and upper extremities, trunk and lower abdomen
Skin involvement is sometimes detected by random skin biopsy of grossly unremarkable skin
Cutaneous variant
– Most frequent in females
– Younger than other IVLBCL patients
– Usually not associated with leucopenia or thrombocytopenia

 .
.