Intravascular Large B-cell Lymphoma
Francisco Vega, MD, PhD
Key Facts
Terminology
Rare large B-cell lymphoma characterized by selective intravascular growth
Clinical Issues
Absence of marked lymphadenopathy
Middle-aged or elderly patients
Predominant neurologic and dermatologic manifestations (Western countries)
Patients from Asia (mainly Japan) preferentially show hemophagocytic syndrome (Asian variant)
Microscopic Pathology
IVLBCL cells are large, with vesicular nuclear chromatin, distinct nucleoli, and frequent mitoses
Lymphoma cells are mainly located in lumina of small vessels
Sinusoidal involvement of liver, spleen, and bone marrow
Ancillary Tests
Pan-B-cell markers(+), Bcl-2(+), MUM1(+)
CD5([+] 30%); other T-cell markers(−)
Ki-67 high
Top Differential Diagnoses
Peripheral T- or NK-cell lymphomas with intravascular pattern
Hepatosplenic T-cell lymphoma
T-cell large granular lymphocytic leukemia
Aggressive NK-cell leukemia/lymphoma
Splenic B-cell marginal zone lymphoma
Diffuse large B-cell lymphoma
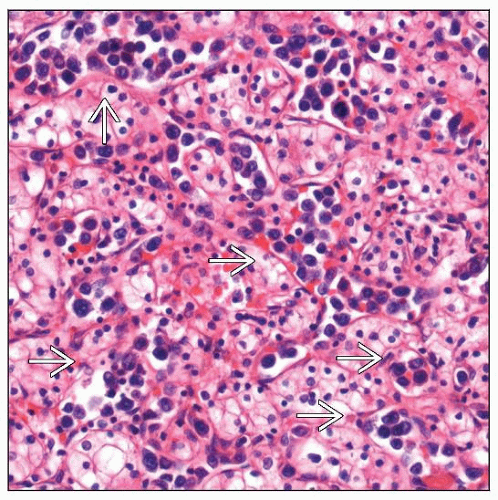 Intravascular large B-cell lymphoma (IVLBCL) in nephrectomy specimen of a patient with renal clear cell carcinoma. Large atypical lymphoid cells are seen inside of small sinusoid-like vessels  . . |
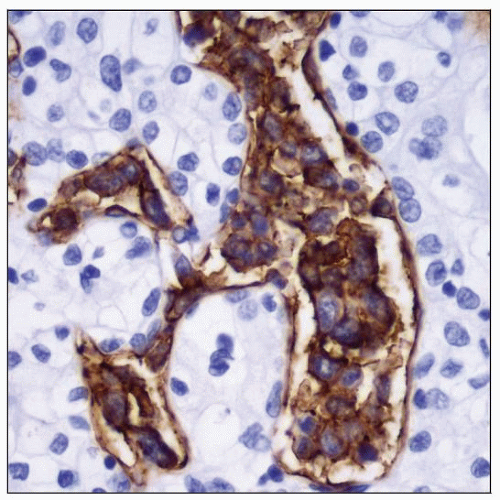 The intravascular large cells are CD20(+) and negative for T-cell antigens (not shown), which supports a B-cell lineage and the diagnosis of IVLBCL. |
TERMINOLOGY
Abbreviations
Intravascular large B-cell lymphoma (IVLBCL)
Synonyms
Angiotropic large cell lymphoma
Angioendotheliotropic (intravascular) lymphoma
Intravascular lymphomatosis
Definitions
Large B-cell lymphoma characterized by selective intravascular growth
Preferential intravascular growth is a conditio sine qua non for diagnosing IVLBCL
Concomitant and minimal extravascular location of neoplastic cells, usually surrounding involved vessels, can be seen
CLINICAL ISSUES
Site
Selective tumor growth within lumina of small blood vessels, particularly capillaries
Widely disseminated
Any organ can be involved
Absence of marked lymphadenopathy
Mechanisms responsible for selective growth of neoplastic cells within blood vessel lumina are unknown
Possible explanations include
Chemokine-chemokine receptor interactions
e.g., CXCL9 (expressed in endothelium) and CXCR3 (expressed in IVLBCL)
Decreased expression of adhesion molecules on surface of IVLBCL cells
e.g., CD29 and CD54
Presentation
Middle-aged or elderly patients; median: 67 years
M:F ratio = 1.3:1
IVLBCL can involve any organ with heterogeneous, often nonspecific symptoms
Fever of unknown origin
General fatigue
Deterioration in performance status
Diagnosis can be clinically difficult and some cases are diagnosed postmortem
2 major patterns of clinical presentation
Western IVLBCL
Predominant neurologic and dermatologic manifestations
Central nervous system is involved in most patients
Asian IVLBCL
Hemophagocytic syndrome
Fever and B symptoms
Pancytopenia and bone marrow infiltration
Skin and central nervous system involvement are uncommon
Skin lesions
Heterogeneous clinical presentation: Plaques, telangiectatic patches, cellulitis, ulcerated nodules
Skin involvement is sometimes detected by random skin biopsy of grossly unremarkable skin
Cutaneous variant
Most frequent in females
Younger than other IVLBCL patients
Better prognosis
Kidney
Increased creatinine
Proteinuria
Renal insufficiency
Liver
Hepatomegaly
Increased bilirubin and liver enzymes
Central nervous system
Alteration of consciousness
Motor and sensory deficits
Seizure
Dementia
Lungs
Dyspnea and hypoxia
Hematopoietic system
Splenomegaly
Hemophagocytosis
Anemia, thrombocytopenia, and leukopenia
Other
Increased LDH
Ascites
Endocrine dysfunction (hypopituitarism)
Multiorgan failure
Treatment
Rituximab-containing chemotherapy plus central nervous system-oriented therapy
R-CHOP plus high-dose methotrexate
Prognosis
Aggressive behavior and often fatal course
Predictive factors that are useful for risk-stratification are not established
MICROSCOPIC PATHOLOGY
Histologic Features
Lymphoma cells are mainly located in lumina of small vessels
Minimal extravascular location of tumor cells can be seen
Usually surrounding involved vessels
Extravascular masses can be detected at autopsy in some patients
Sinusoidal involvement of liver, spleen, and bone marrow
Spleen: Red pulp involvement
Kidney: Neoplastic cells within glomerular capillaries and peritubular capillaries
Brain: Neoplastic cells within small vessels
Circulating lymphoma cells can be occasionally seen in peripheral blood
Fibrin thrombi, hemorrhage, and necrosis
Cytologic Features
Usually tumor cells are large, with vesicular nuclear chromatin with distinct nucleoli
In some cases, tumor cells have coarse nuclear chromatin and irregular or indented nuclei
Mitoses are frequent
IVLBCL cell size may be smaller than usual in some cases
ANCILLARY TESTS
Immunohistochemistry
Pan-B-cell markers(+)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


