Patient Stories
A young woman presented to the office with a 3-day history of an uncomfortable rash on her lip and chin (Figure 116-1). She denied any trauma or previous history of oral herpes. This case of impetigo resolved quickly with oral cephalexin.

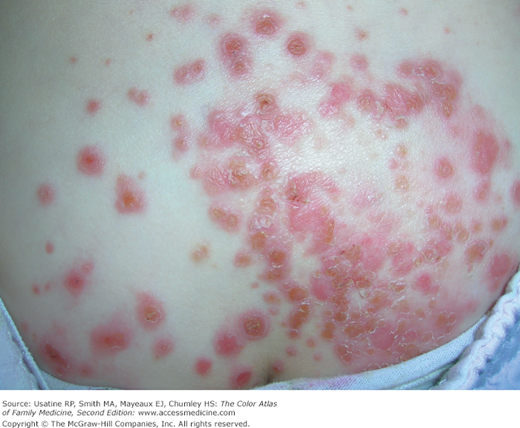
An 11-year-old-child presented with a 5-day history of a skin lesion that started after a hiking trip (Figure 116-2). This episode of bullous impetigo was found to be secondary to methicillin-resistant Staphylococcus aureus (MRSA). The lesion was rapidly progressive and was developing a surrounding cellulitis. She was admitted to a hospital and treated with intravenous clindamycin with good results.1
Figure 116-2

Bullous impetigo secondary to methicillin-resistant Staphylococcus aureus (MRSA) on the leg of an 11-year-old child. Note the surrounding cellulitis. (With permission from Studdiford J, Stonehouse A. Bullous eruption on the posterior thigh 1. J Fam Pract. 2005;54:1041-1044. Reproduced with permission from Frontline Medical Communications.)
Introduction
Epidemiology
Etiology and Pathophysiology
Diagnosis
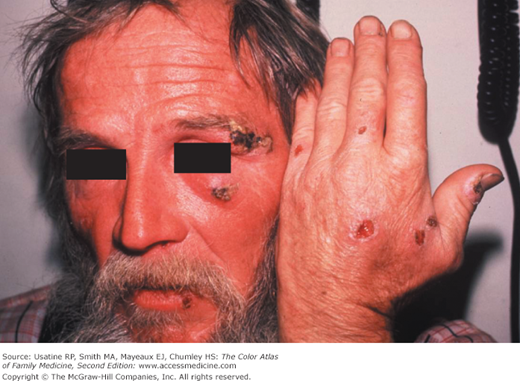
- Vesicles, pustules, honey-colored (Figure 116-1), brown or dark crusts, erythematous erosions (Figure 116-3), ulcers in ecthyma (Figure 116-4), bullae in bullous impetigo (Figures 116-5, 116-6, 116-7).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


