2 most common mutations (C282Y and H63D) account for vast majority of cases
• Non- HFE- associated hereditary hemochromatosis occurs less commonly (5-10% of phenotypic cases)
• Specific mechanism leading to iron overload in HH is still unknown
Clinical Issues
• Most patients are of Northern European ancestry
• Highly variable clinical presentation
Presenting signs/symptoms include weakness, evidence of liver disease, cardiac dysfunction, diabetes, skin hyperpigmentation
• Phlebotomy is mainstay of treatment
• Patients are at increased risk for hepatocellular carcinoma, even in absence of cirrhosis and adequate iron-depletion therapy
Macroscopic
• Dark, rusty brown discoloration
Microscopic
• Iron deposition is characteristic feature
Initially in zone 1 hepatocytes, but progresses to involve all zones
May also be present in macrophages, biliary epithelium
Ancillary Tests
• Molecular testing for individual mutations
• Liver biopsy with measurement of quantitative iron and hepatic iron index
• Serum iron indices
Gross Appearance This liver obtained from a hereditary hemochromatosis (HH) patient at autopsy shows the characteristic rust-brown color that is typical of increased iron deposition. (Courtesy G. Gray, Jr., MD.)
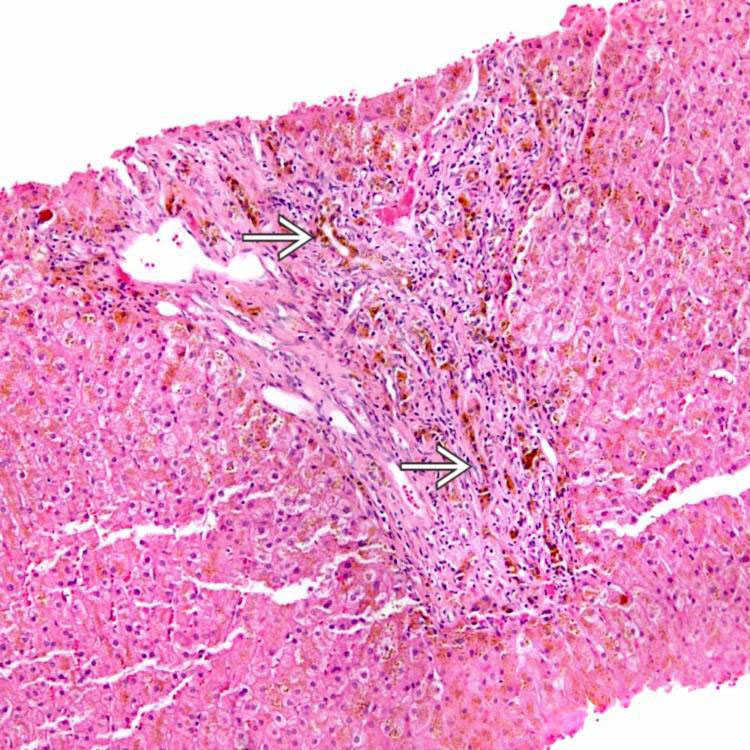
Periportal Iron Deposition Iron deposition is visible on a routine H&E stain from this biopsy. Note the periportal iron deposition as well as iron in the bile ducts and ductules .
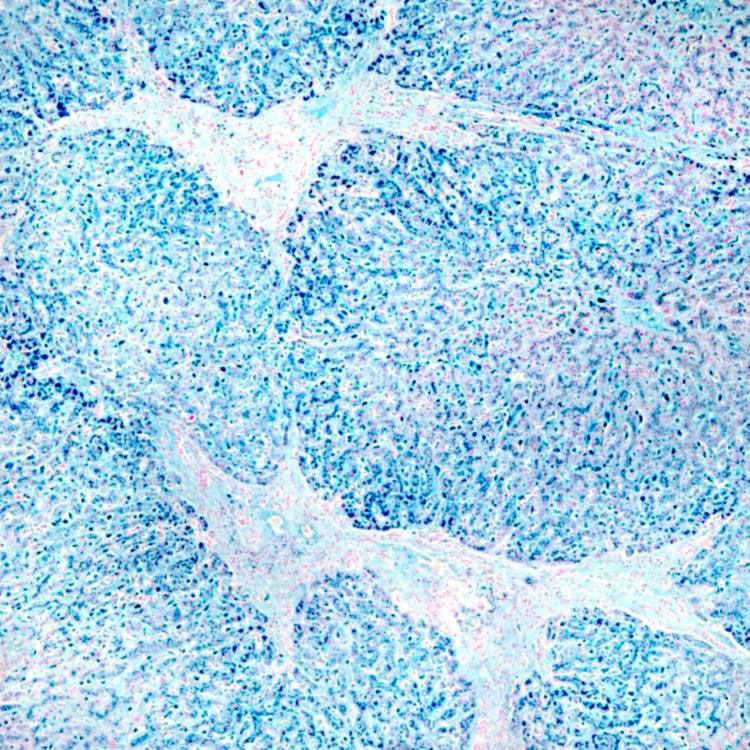
Iron Stain, Cirrhosis Prussian blue iron stain highlights extensive iron deposition in the hepatocytes of cirrhotic nodules, as well as in the Kupffer cells.
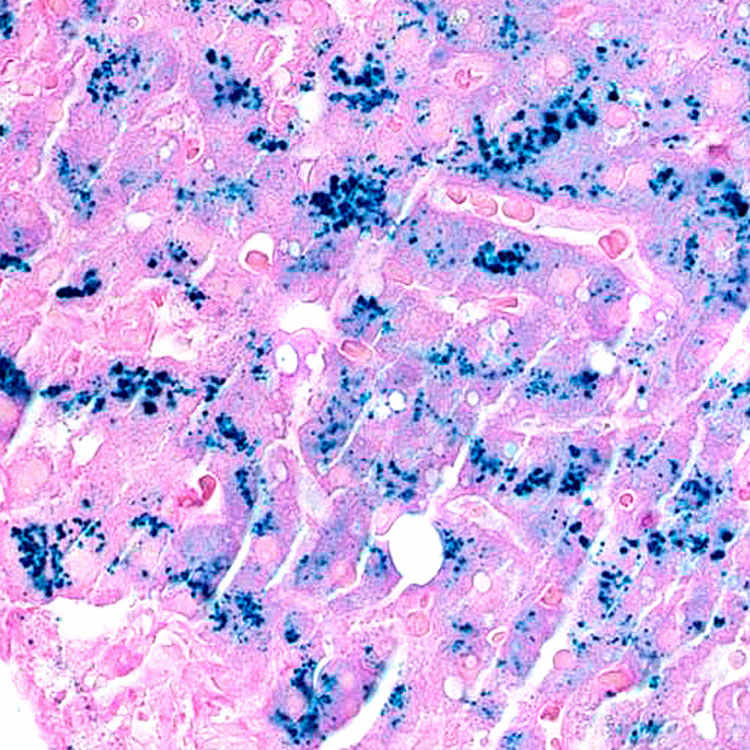
Iron Stain, Pericanalicular Pattern Perl iron stain shows the pericanalicular pattern of iron deposition in the hepatocytes, typical of most HH.
TERMINOLOGY
Abbreviations
• Hereditary hemochromatosis (HH)
Definitions
• Inherited, autosomal recessive disorder of iron metabolism
Extremely variable penetrance and phenotypic expression
ETIOLOGY/PATHOGENESIS
Genetic Mutations
• 2 most common mutations are in HFE gene
C282Y/C282Y homozygotes
– 80-85% of phenotypic cases
Compound C282Y/H63D heterozygotes
– 5% of phenotypic cases
• Non- HFE- associated HH occurs less commonly
5-10% of phenotypic cases
TFR2 (transferrin receptor) mutations
Ferroportin mutations
Juvenile hemochromatosis
– Rare
– Progresses rapidly and leads to significant disease before age 30
– Lower frequency of liver disease
• Specific mechanism leading to iron overload in HH is still unknown
CLINICAL ISSUES
Epidemiology
• Incidence
Worldwide allele frequencies
– C282Y: 1.9%
– H63D: 8.1%
• Ethnicity
Most often Northern European origin
– C282Y frequency higher in Irish individuals
– H63D frequency higher in Basque individuals
Presentation
• 4 clinical stages
Genetic predisposition with no clinical or laboratory abnormality
Mild iron overload without clinical abnormality
Only gold members can continue reading. Log In or Register to continue




 .
.