Pure fetal epithelial histology is associated with favorable prognosis
Embryonal and fetal epithelial patterns often seen together
Macrotrabecular is composed of fetal or embryonal type cells in wide trabeculae
Small undifferentiated component is associated with poorer prognosis
• Mixed hepatoblastoma (HB) are composed of epithelial and mesenchymal components
Mesenchymal component can range from immature spindle cells to fibrous tissue
Osteoid-like and teratoid elements can occur
Ancillary Tests
• Nuclear β-catenin staining in epithelial and mesenchymal components (70% of cases), often membranous in fetal pattern
• Positive glypican-3 and Hep-Par1 staining in fetal and embryonal epithelial cells
• Positive glutamine synthetase staining in fetal and variably in embryonal cells
Top Differential Diagnoses
• Normal liver parenchyma; positive nuclear &/or cytoplasmic β-catenin staining in HB
• Hepatocellular carcinoma; presence of both fetal and embryonal patterns diagnostic of HB
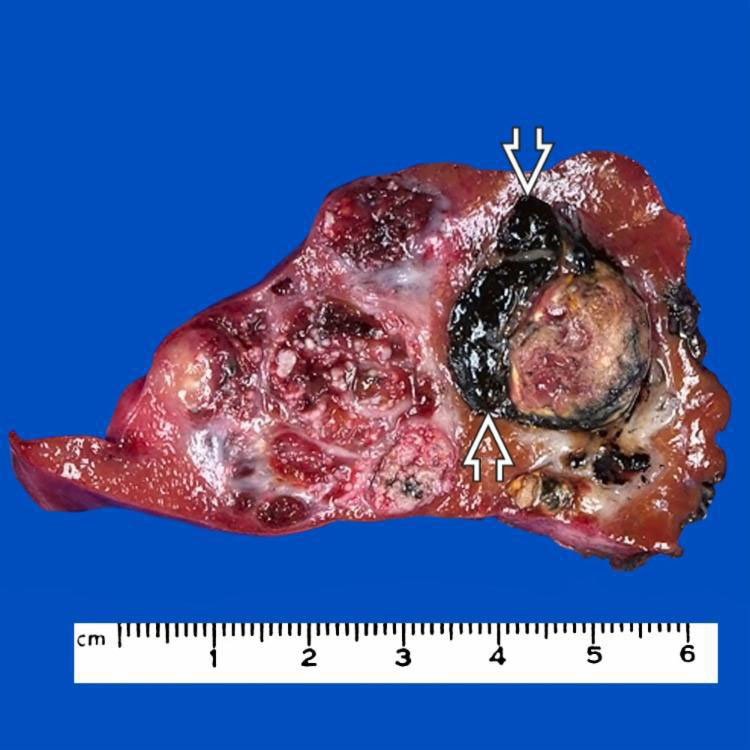
Treated Hepatoblastoma, Gross This tumor was treated with preoperative chemotherapy and was diagnosed as a mixed epithelial and mesenchymal hepatoblastoma with teratoid features. The black focus contained melanin pigment.
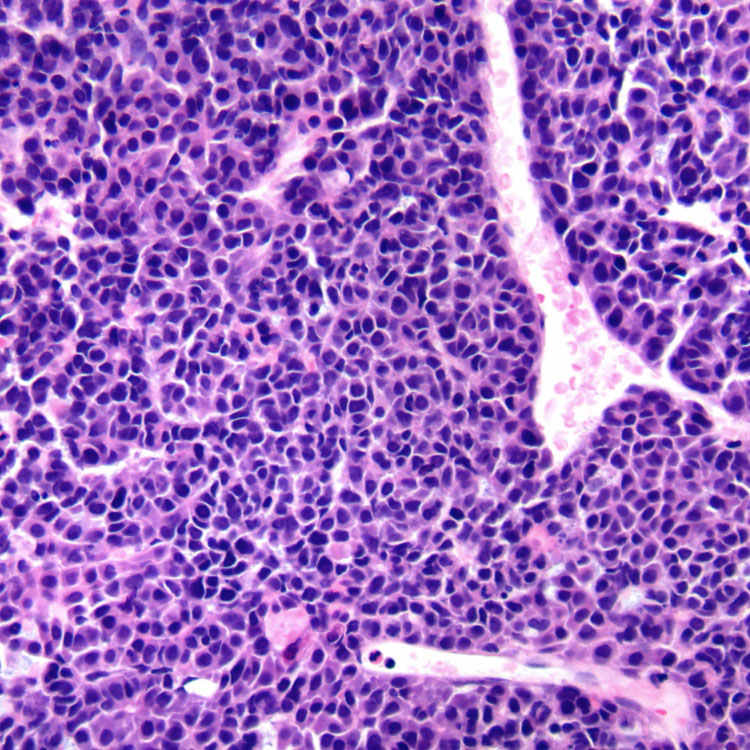
Embryonal Pattern H&E shows sheets and poorly formed nests of embryonal epithelial cells with angulated nuclei and less cytoplasm than fetal epithelial cells, which can often coexist in the same tumor. Embryonal cells have nuclear or cytoplasmic reactivity to β-catenin and are diffusely positive for glypican-3.
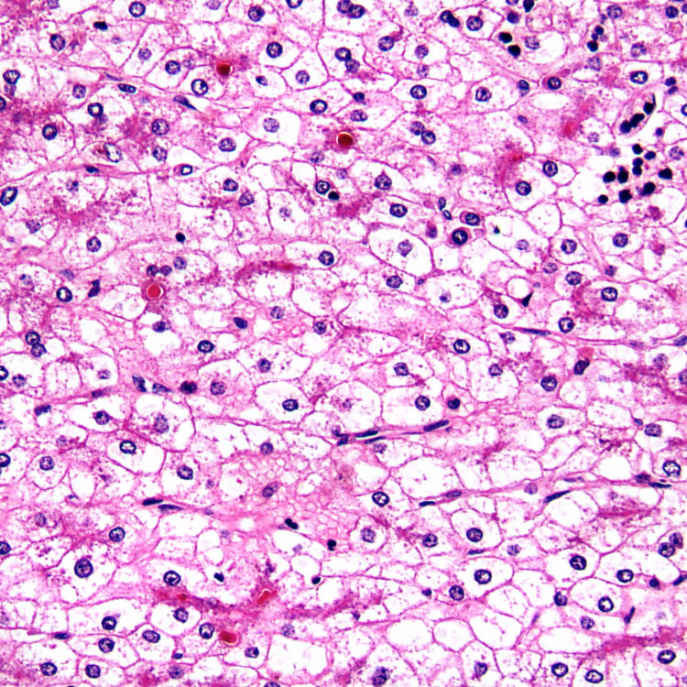
Pure Fetal Histology H&E shows uniform polygonal cells that are smaller than normal hepatocytes with round nuclei, no nucleoli, clear cytoplasm, and no mitotic activity.
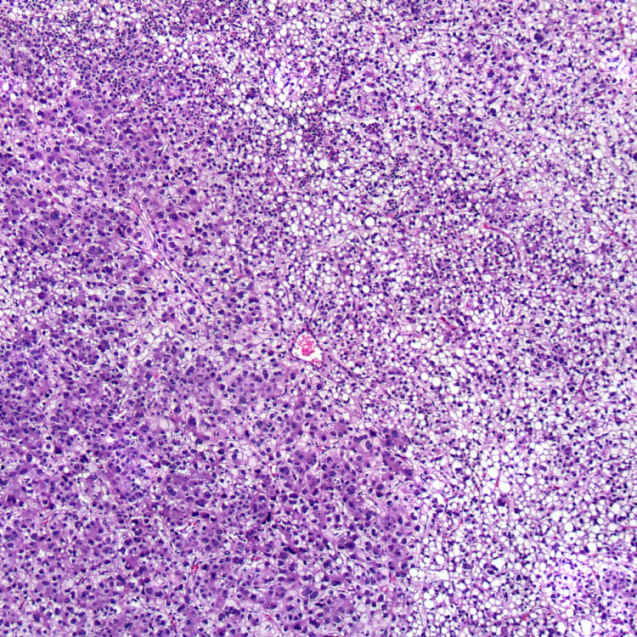
Pure Fetal Histology Light and dark appearance is due to variable amounts of glycogen or cytoplasmic lipid. If the entire tumor has this appearance and mitotic activity ≤ 2/10 HPF, it would be classified as pure fetal histology.
TERMINOLOGY
Abbreviations
• Hepatoblastoma (HB)
Definitions
• Predominantly pediatric liver tumor that mimics developing fetal or embryonal liver histologically
ETIOLOGY/PATHOGENESIS
Neoplasm
• Wnt pathway activation in 70-90% due to β-catenin mutation
CLINICAL ISSUES
Epidemiology
• Incidence
2.1% of all pediatric cancers (1-19 years)
Higher in low birth weight infants
• Age
Most common malignant liver neoplasm in children
– 88% in children ≤ 5 years and 3% > 15 years
– Mean age at diagnosis is 19 months
• Sex
Male predominance (M:F = 3:2)
Site
• 58% involve right lobe, 27% involve both lobes
Presentation
• Painless abdominal mass, hepatomegaly
Laboratory Tests
• Increased serum α-fetoprotein in 75-96% of patients
Often ≥ 100,000 ng/mL
Caveat: High AFP normal before 6 months of age
Useful marker of response to therapy and recurrence
Treatment
• Surgical resection
Stage 1 pure fetal HB cured by surgical resection alone
Only 1/3 to 1/2 have resectable disease at presentation
Preoperative chemotherapy converts > 50% of inoperable tumors to resectable tumors
Children’s Oncology Group (COG) standard regimen consists of cisplatin, 5-fluorouracil, and vincristine (C5V)
• Liver transplant considered in unresectable cases
COG Staging System (Pretreatment Staging)
• Stage I: Completely resected tumor with negative margin





 contained melanin pigment.
contained melanin pigment.