Portal vein thrombosis, systemic inflammatory conditions, some neoplasms such as renal cell carcinoma or lymphoma, artifactual sinusoidal dilatation
• Other causes of parenchymal necrosis/hemorrhage
Acetaminophen toxicity, ischemic liver injury
Sinusoidal Dilatation In Budd-Chiari syndrome, increased sinusoidal pressure causes sinusoidal dilatation, congestion , and hepatocellular atrophy .
RBC in Space of Disse Extravasation of RBC in the space of Disse (the potential space between the hepatocytes and sinusoidal basement membrane) is caused by increased sinusoidal pressure.
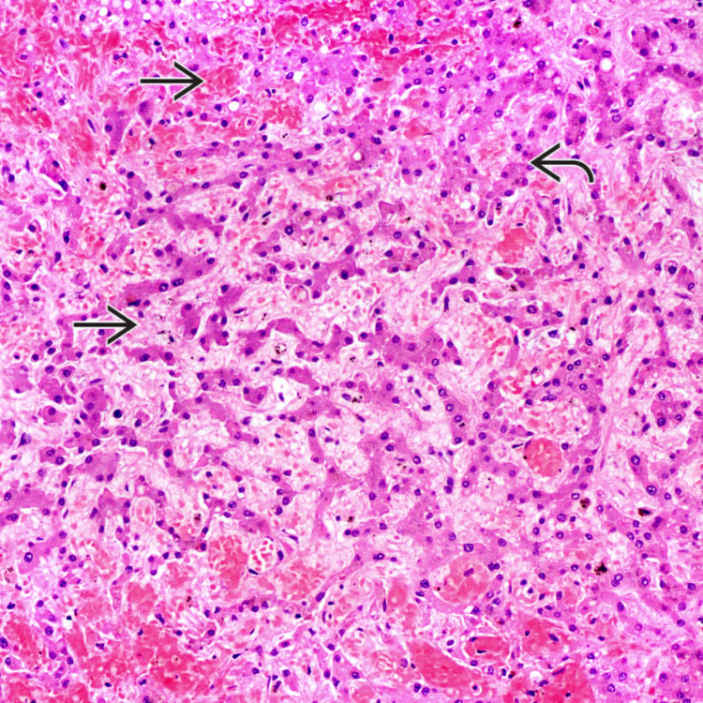
Hemorrhagic Necrosis Hepatocellular necrosis around the central vein can be seen in HVOO, especially in cases presenting acutely. Inflammation is typically mild or absent, unlike centrizonal necrosis seen in autoimmune hepatitis or adverse drug reaction.
Ductular Reaction Ductular reaction can be seen in portal tracts as well as centrizonal regions. It is generally mild in portal areas but can be prominent and accompanied by portal inflammation &/or focal bile duct damage. These findings can closely mimic biliary disease.
TERMINOLOGY
Abbreviations
• Hepatic venous outflow obstruction (HVOO)
ETIOLOGY/PATHOGENESIS
Venous Obstruction
• Can occur at different levels of hepatic venous outflow
Sinusoids or small hepatic veins: Sinusoidal obstruction syndrome (formerly venoocclusive disease)
Large hepatic veins or inferior vena cava [Budd-Chiari syndrome (BCS)]
Right heart or pericardial disease
– Right heart failure (either isolated or result of left heart failure)
– Tricuspid valve disease
– Cardiac amyloidosis
– Constrictive pericarditis
Pathogenesis
• Liver changes result from hepatic venous congestion, increased hepatic and sinusoidal pressure, and necrosis
• Secondary sinusoidal thrombosis extending into hepatic and portal veins may contribute to parenchymal damage and fibrosis
CLINICAL ISSUES
Presentation
• Subacute presentation (< 6 months) is most common with painful hepatomegaly, mild jaundice, and ascites
• Less commonly, presents as chronic liver disease or cirrhosis
• Rare cases have fulminant presentation with acute liver failure
Laboratory Tests
• Mild elevation of transaminases; marked increase in acute cases
• Alkaline phosphatase elevation is common
Treatment
• Decompression procedures in BCS
Nonsurgical decompression by percutaneous transluminal angioplasty with stent: Suitable for webs or limited stenosis

 , and hepatocellular atrophy
, and hepatocellular atrophy  .
.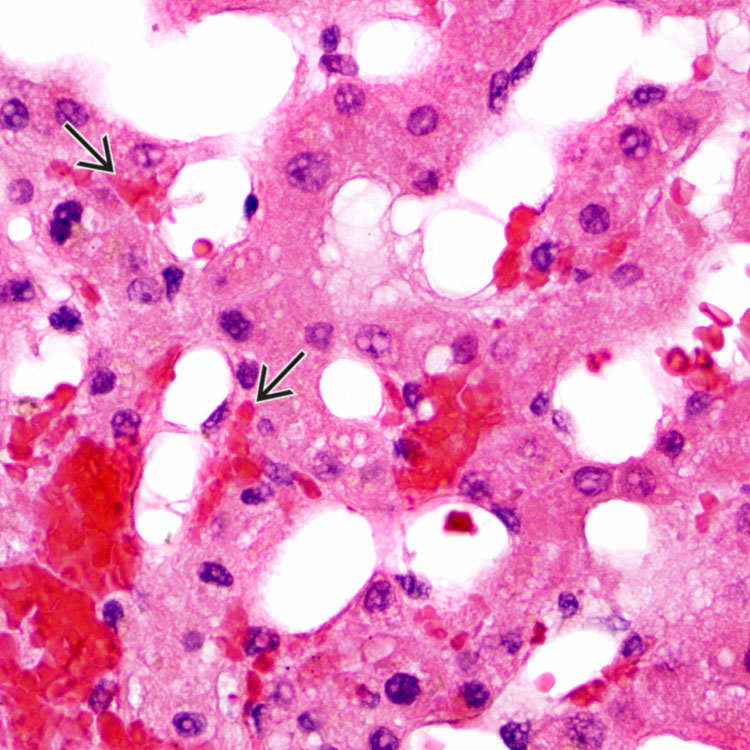
 in the space of Disse (the potential space between the hepatocytes and sinusoidal basement membrane) is caused by increased sinusoidal pressure.
in the space of Disse (the potential space between the hepatocytes and sinusoidal basement membrane) is caused by increased sinusoidal pressure.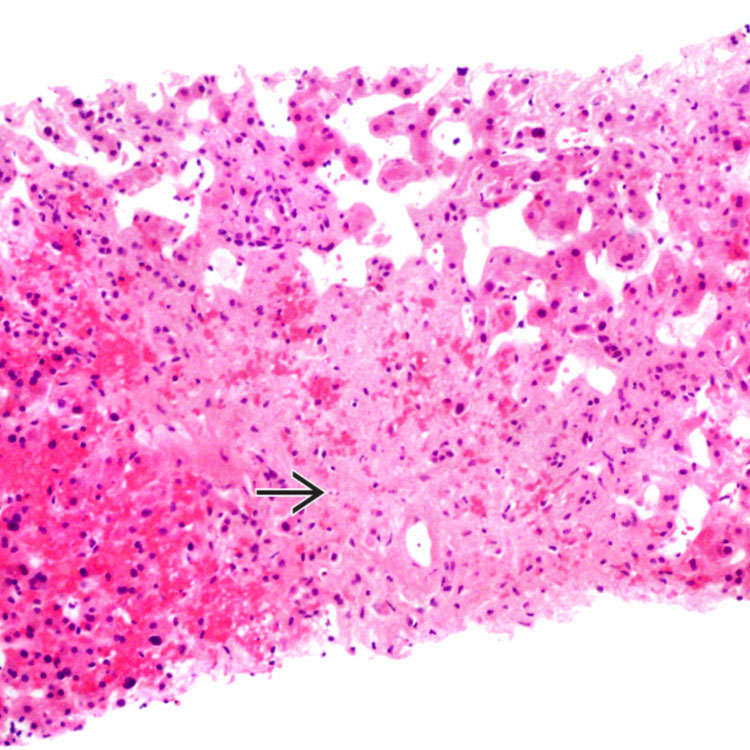
 around the central vein can be seen in HVOO, especially in cases presenting acutely. Inflammation is typically mild or absent, unlike centrizonal necrosis seen in autoimmune hepatitis or adverse drug reaction.
around the central vein can be seen in HVOO, especially in cases presenting acutely. Inflammation is typically mild or absent, unlike centrizonal necrosis seen in autoimmune hepatitis or adverse drug reaction.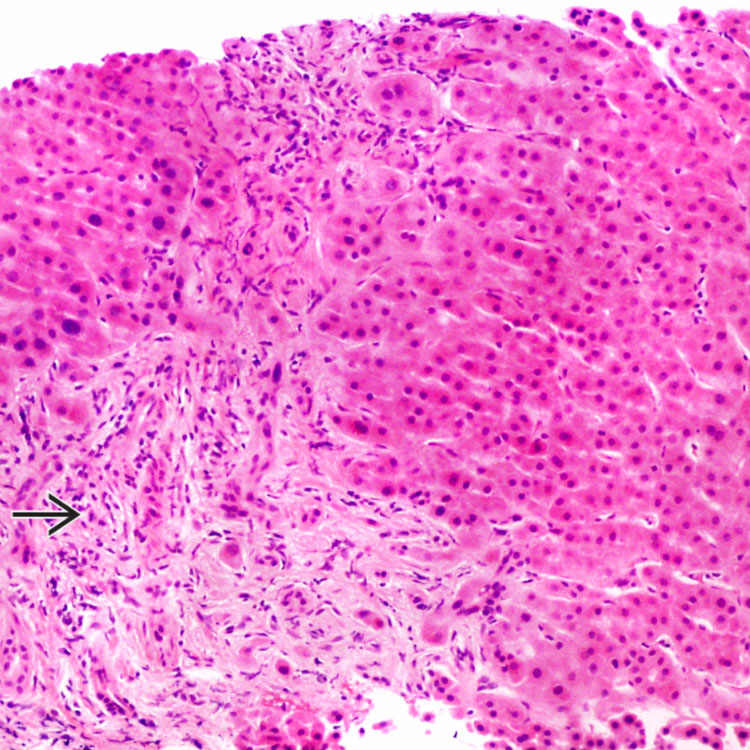
 can be seen in portal tracts as well as centrizonal regions. It is generally mild in portal areas but can be prominent and accompanied by portal inflammation &/or focal bile duct damage. These findings can closely mimic biliary disease.
can be seen in portal tracts as well as centrizonal regions. It is generally mild in portal areas but can be prominent and accompanied by portal inflammation &/or focal bile duct damage. These findings can closely mimic biliary disease.














