According to the World Tourism Organization, international tourist arrivals grew dramatically from 25 million in 1950 to >1 billion in 2012. Not only are more people traveling; travelers are seeking more exotic and remote destinations. Travel from industrialized to developing regions has been increasing, with Asia and the Pacific, Africa, and the Middle East now emerging destinations. Figure 149-1 summarizes the monthly incidence of health problems during travel in developing countries. Studies continue to show that 50–75% of short-term travelers to the tropics or subtropics report some health impairment. Most of these health problems are minor: only 5% require medical attention, and <1% require hospitalization. Although infectious agents contribute substantially to morbidity among travelers, these pathogens account for only ~1% of deaths in this population. Cardiovascular disease and injuries are the most frequent causes of death among travelers from the United States, accounting for 49% and 22% of deaths, respectively. Age-specific rates of death due to cardiovascular disease are similar among travelers and nontravelers. In contrast, rates of death due to injury (the majority from motor vehicle, drowning, or aircraft accidents) are several times higher among travelers. Motor vehicle accidents account for >40% of travelers’ deaths that are not due to cardiovascular disease or preexisting illness.
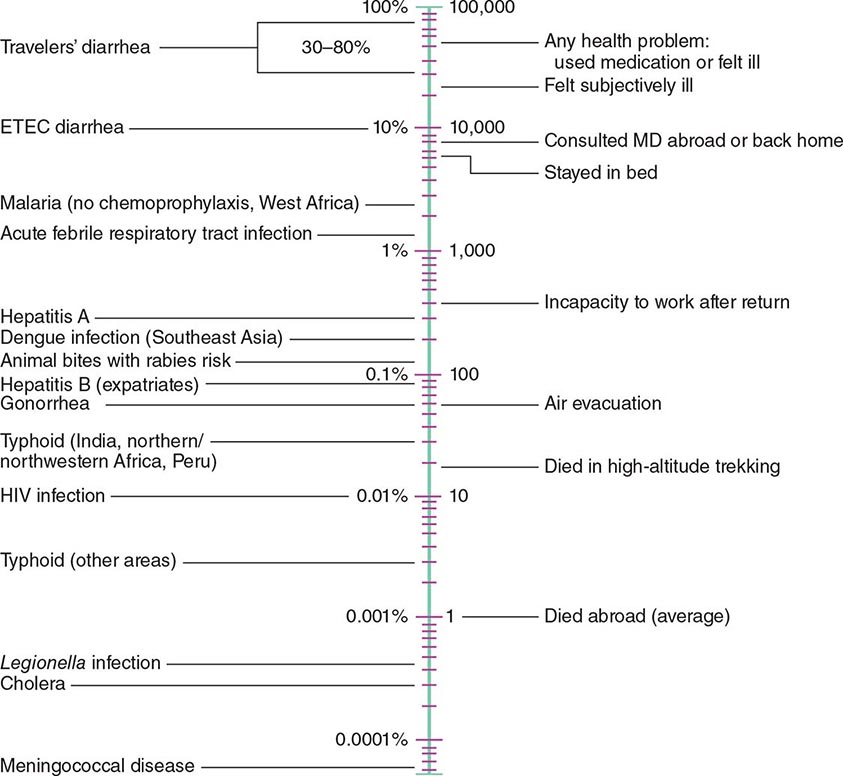
FIGURE 149-1 Monthly incidence rates of health problems during stays in developing countries. ETEC, enterotoxigenic Escherichia coli. (From R Steffen et al: Int J Antimicrob Agents 21:89, 2003.)
GENERAL ADVICE
Health maintenance recommendations are based not only on the traveler’s destination but also on assessment of risk, which is determined by such variables as health status, specific itinerary, purpose of travel, season, and lifestyle during travel. Detailed information regarding country-specific risks and recommendations may be obtained from the Centers for Disease Control and Prevention (CDC) publication Health Information for International Travel (available at www.cdc.gov/travel).
Fitness for travel is an issue of growing concern in view of the increased numbers of elderly and chronically ill individuals journeying to exotic destinations (see “Travel and Special Hosts,” below). Since most commercial aircraft are pressurized to 2500 m (8000 ft) above sea level (corresponding to a Pa02 of ~55 mmHg), individuals with serious cardiopulmonary problems or anemia should be evaluated before travel. In addition, those who have recently had surgery, a myocardial infarction, a cerebrovascular accident, or a deep-vein thrombosis may be at high risk for adverse events during flight. A summary of current recommendations regarding fitness to fly has been published by the Aerospace Medical Association Air Transport Medicine Committee (www.asma.org/publications/medical-publications-for-airline-travel). A pretravel health assessment may be advisable for individuals considering particularly adventurous recreational activities, such as mountain climbing and scuba diving.
IMMUNIZATIONS FOR TRAVEL
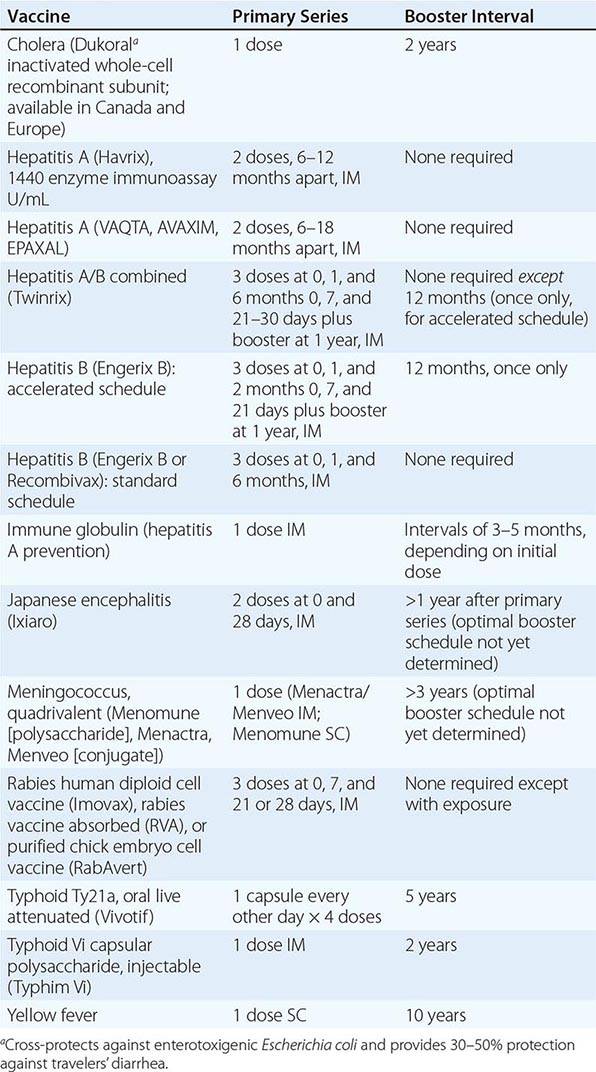
Immunizations for travel fall into three broad categories: routine (childhood/adult boosters that are necessary regardless of travel), required (immunizations that are mandated by international regulations for entry into certain areas or for border crossings), and recommended (immunizations that are desirable because of travel-related risks). Required and recommended vaccines commonly given to travelers are listed in Table 149-1.
VACCINES COMMONLY USED FOR TRAVEL IN ADULTS |
Routine Immunizations • DIPHTHERIA, TETANUS, AND POLIO Diphtheria (Chap. 175) continues to be a problem worldwide. Large outbreaks have occurred in countries that do not have rigorous vaccination programs or that have reduced their public vaccination programs. Serologic surveys show that tetanus (Chap. 177) antibodies are lacking in many North Americans, especially in women over the age of 50. The risk of polio (Chap. 228) to the international traveler is extremely low, and wild-type poliovirus has been eradicated from the Western Hemisphere and Europe. However, studies in the United States suggest that 12% of adult travelers are unprotected against at least one poliovirus serogroup. In addition, challenges continue to be faced by polio eradication programs. Foreign travel offers an ideal opportunity to have these immunizations updated. With the recent increase in pertussis among adults, the diphtheria–tetanus–acellular pertussis (Tdap) combination is now recommended for adults as a once-only replacement for the 10-year tetanus–diphtheria (Td) booster.
MEASLES Measles (rubeola) continues to be a major cause of morbidity and death in the developing world (Chap. 229). Several outbreaks of measles in the United States and Canada have been linked to imported cases, especially from Europe, where large outbreaks have occurred recently. The group at highest risk consists of persons born after 1956 and vaccinated before 1980, in many of whom primary vaccination failed. The measles–mumps–rubella (MMR) vaccine is typically used; its coverage of rubella also addresses a growing concern in some areas of Eastern Europe and Asia.
INFLUENZA Influenza (Chap. 224)—possibly the most common vaccine-preventable infection in travelers—occurs year-round in the tropics and during the summer months in the Southern Hemisphere (coinciding with the winter months in the Northern Hemisphere). One prospective study showed that influenza developed in 1% of travelers to Southeast Asia per month of stay. Annual vaccination should be considered for all travelers who do not have a contraindication. Travel-related influenza continues to occur during summer months in Alaska and the Northwest Territories of Canada among cruise-ship passengers and staff. The speed of global spread of the pandemic H1N1 virus once again illustrates why influenza immunization is so important for travelers.
PNEUMOCOCCAL INFECTION Regardless of travel, pneumococcal vaccine (Chap. 171) should be administered routinely to persons over the age of 65 and to persons at high risk of serious infection, including those with chronic heart, lung, or kidney disease; those who have been splenectomized; and those who have sickle cell disease.
Required Immunizations • YELLOW FEVER Documentation of vaccination against yellow fever (Chap. 233) may be required or recommended as a condition for entry into or passage through countries of sub-Saharan Africa and equatorial South America, where the disease is endemic or epidemic, or (by the International Health Regulations) for entry into countries at risk of having the infection introduced. This vaccine is given only by state-authorized yellow fever centers, and its administration must be documented on an official International Certificate of Vaccination. A registry of U.S. clinics that provide the vaccine is available from the CDC (www.cdc.gov/travel). Recent data suggest that fewer than 50% of travelers entering areas endemic for yellow fever are immunized; this lack of coverage is a serious problem, as 13 countries in Central and South America and 30 countries in Africa harbor the illness. Severe adverse events associated with this vaccine have recently increased in incidence. First-time vaccine recipients may present with a syndrome characterized as either neurotropic (1 case per 125,000 doses) or viscerotropic (overall, 1 case per 250,000 doses; among persons 60–69 years of age, 1 case per 100,000 doses; and among persons ≥ 70 years of age, 1 case per 40,000 doses). Immunosuppression and thymic disease increase the risk of these adverse events (www.cdc.gov/vaccines/hcp/vis/vis-statements/yf.pdf).
MENINGOCOCCAL MENINGITIS Protection against meningitis with one of the quadrivalent (preferably conjugate) vaccines is required for entry into Saudi Arabia during the Hajj (Chap. 180).
INFLUENZA Both seasonal and pandemic H1N1 vaccines (the latter, where available) were required for entry into Saudi Arabia during the Hajj in 2013.
Recommended Immunizations • HEPATITIS A AND B Hepatitis A (Chap. 360) is one of the most common vaccine-preventable infections of travelers. The risk is six times greater for travelers who stray from the usual tourist routes. The mortality rate for hepatitis A increases with age, reaching almost 2% among individuals over age 50. Of the four hepatitis A vaccines currently available in North America (two in the United States), all are interchangeable and have an efficacy of >95%. Hepatitis A vaccine is currently given to all children in the United States. Since the most frequently identified risk factor for hepatitis A in the United States is international travel, and since morbidity and mortality increase with age, it seems appropriate that all adults be immune prior to travel.
Long-stay overseas workers appear to be at considerable risk for hepatitis B infection (Chap. 360). The recommendation that all travelers be immunized against hepatitis B before departure is supported by two studies showing that 17% of the assessed travelers who received health care abroad had some type of injection; according to the World Health Organization, nonsterile equipment is used for up to 75% of all injections given in parts of the developing world. A 3-week accelerated schedule of the combined hepatitis A and B vaccine has been approved in the United States. Although no data are available on the specific risk of infection with hepatitis B virus among U.S. travelers, ~240 million people in the world have chronic infection. All children and adolescents in the United States are immunized against this illness. Hepatitis B vaccination should be considered for all travelers.
TYPHOID FEVER Most cases of typhoid fever in North America are due to travel, with ~300 cases seen per year in the United States. The attack rate for typhoid fever (Chap. 190) is 1 case per 30,000 travelers per month of travel to the developing world. However, attack rates in India, Senegal, and North Africa are tenfold higher; rates are especially high among travelers to relatively remote destinations and among immigrants and their families who have returned to their homelands to visit friends or relatives (VFRs). Between 1999 and 2006 in the United States, 66% of imported cases involved the latter group. Unfortunately, data show that the causative organism has become increasingly resistant to fluoroquinolone antibiotics (especially in those cases acquired on the Indian subcontinent). Both of the available vaccines—one oral (live) and the other injectable (polysaccharide)—have efficacy rates of ~70%. In some countries, a combined hepatitis A/typhoid vaccine is available.
MENINGOCOCCAL MENINGITIS Although the risk of meningococcal disease among travelers has not been quantified, it is likely to be higher among travelers who live with poor indigenous populations in overcrowded conditions (Chap. 180). Because of its enhanced ability to prevent nasal carriage (compared with the older polysaccharide vaccine), a quadrivalent conjugate vaccine is the product of choice (regardless of age) for immunization of persons traveling to sub-Saharan Africa during the dry season or to areas of the world where there are epidemics. The vaccine, which protects against serogroups A, C, Y, and W-135, has an efficacy rate of >90%.
JAPANESE ENCEPHALITIS The risk of Japanese encephalitis (Chap. 233), an infection transmitted by mosquitoes in rural Asia and Southeast Asia, can be as high as ~1 case per 5000 travelers per month of stay in an endemic area. Most infections are asymptomatic, with a very small proportion of infected persons becoming ill. However, among those who do become ill, severe neurologic sequelae are common. Most symptomatic infections among U.S. residents have involved military personnel or their families. The vaccine efficacy rate is >90%. The vaccine is recommended for persons staying >1 month in rural endemic areas or for shorter periods if their activities (e.g., camping, bicycling, hiking) in these areas will increase exposure risk.
CHOLERA The risk of cholera (Chap. 193) is extremely low, with ~1 case per 500,000 journeys to endemic areas. Cholera vaccine, not currently available in the United States, was rarely recommended but was considered for aid and health care workers in refugee camps or in disaster-stricken/war-torn areas. A more effective oral cholera vaccine is available in other countries.
RABIES Domestic animals, primarily dogs, are the major transmitters of rabies in developing countries (Chap. 232). Several studies have shown that the risk of rabies posed by a dog bite in an endemic area translates into 1–3.6 cases per 1000 travelers per month of stay. Countries where canine rabies is highly endemic include Mexico, the Philippines, Sri Lanka, India, Thailand, China, and Vietnam. The two vaccines available in the United States provide >90% protection. Rabies vaccine is recommended for long-stay travelers, particularly children (who tend to play with animals and may not report bites), and for persons who may be occupationally exposed to rabies in endemic areas; however, in a large-scale study, almost 50% of potential exposures occurred within the first month of travel. Even after receipt of a preexposure rabies vaccine series, two postexposure doses are required. Travelers who have had the preexposure series do not require rabies immune globulin (which is often unavailable in developing countries) if they are exposed to the disease.
PREVENTION OF MALARIA AND OTHER INSECT-BORNE DISEASES
It is estimated that more than 30,000 American and European travelers develop malaria each year (Chap. 248). The risk to travelers is highest in Oceania and sub-Saharan Africa (estimated at 1:5 and 1:50 per month of stay, respectively, among persons not using chemoprophylaxis); intermediate in malarious areas on the Indian subcontinent and in Southeast Asia (1:250–1:1000 per month); and low in South and Central America (1:2500–1:10,000 per month). Of the 1925 cases of malaria reported in 2011 in the United States (the highest figure in 40 years), 90% of those due to Plasmodium falciparum occurred in travelers returning or emigrating from Africa and Oceania. VFRs are at the highest risk of acquiring malaria and may die of the disease if their immunity has waned after living outside an endemic area for a number of years. According to data from the CDC, VFRs accounted for 59% of severe malaria cases in the United States in 2011. With the worldwide increase in chloroquine- and multidrug-resistant falciparum malaria, decisions about chemoprophylaxis have become more difficult. The case-fatality rate for falciparum malaria in the United States is 4%; however, in only one-third of patients who die is the diagnosis of malaria considered before death.
Several studies indicate that fewer than 50% of travelers adhere to basic recommendations for malaria prevention. Keys to the prevention of malaria include both personal protection measures against mosquito bites (especially between dusk and dawn) and malaria chemoprophylaxis. The former measures entail the use of DEET-containing insect repellents, permethrin-impregnated bed nets and clothing, screened sleeping accommodations, and protective clothing. Thus, in regions where infections such as malaria are transmitted, DEET products (25–50%) are recommended, even for children and infants at birth. Studies suggest that concentrations of DEET above ~50% do not offer a marked increase in protection time against mosquitoes. The CDC also recommends picaridin, oil of lemon eucalyptus (PMD, para-menthane-3,8-diol), and IR3535 (3-[N-butyl-N-acetyl]-aminopropionic acid, ethyl ester). In general, higher concentrations of any active ingredient provide a longer duration of protection. Personal protection measures also help prevent other insect-transmitted illnesses, such as dengue fever (Chap. 233). Over the past decade, the incidence of dengue has markedly increased, particularly in the Caribbean region, Latin America, Southeast Asia, and (more recently) Africa. Chikungunya, another mosquito-borne infection that clinically resembles dengue fever but with arthralgia and arthritis instead of myalgia, has recently crossed to the Western Hemisphere; many thousands of cases are now occurring in the Caribbean. Both dengue and chikungunya viruses are transmitted by an urban-dwelling mosquito that bites primarily at dawn and dusk.
Table 149-2 lists the currently recommended drugs of choice for prophylaxis of malaria, by destination.
MALARIA CHEMOSUPPRESSIVE REGIMENS, ACCORDING TO GEOGRAPHIC AREAa |
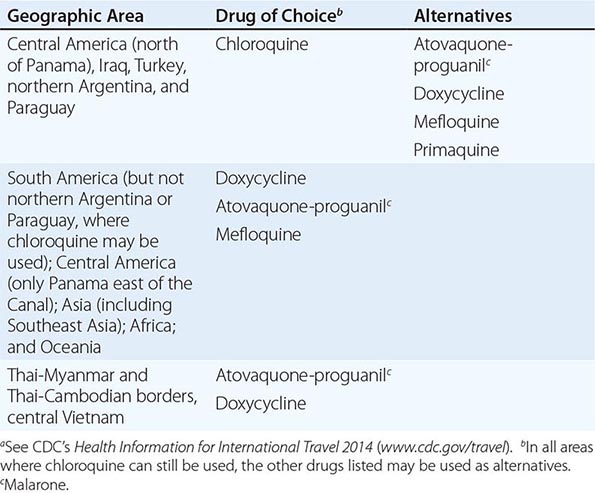
Note: See also Chap. 248.
PREVENTION OF GASTROINTESTINAL ILLNESS
Diarrhea, the leading cause of illness in travelers (Chap. 160), is usually a short-lived, self-limited condition. However, 40% of affected individuals need to alter their scheduled activities, and another 20% are confined to bed. The most important determinant of risk is the destination. Incidence rates per 2-week stay have been reported to be as low as 8% in industrialized countries and as high as 55% in parts of Africa, Central and South America, and Southeast Asia. Infants and young adults are at particularly high risk for gastrointestinal illness and for complications such as dehydration. Recent reviews suggest that there is little correlation between dietary indiscretions and the occurrence of travelers’ diarrhea. Earlier studies of U.S. students in Mexico showed that eating meals in restaurants and cafeterias or consuming food from street vendors was associated with increased risk. For further discussion, see “Precautions,” below.
Etiology (See also Table 160-3) The most frequently identified pathogens causing travelers’ diarrhea are enterotoxigenic and enteroaggregative Escherichia coli (Chap. 186), although in some parts of the world (notably northern Africa and Southeast Asia) Campylobacter infections (Chap. 192) appear to predominate. Other common causative organisms include Salmonella (Chap. 190), Shigella (Chap. 191), rotavirus (Chap. 227), and norovirus (Chap. 227). The latter virus has caused numerous outbreaks on cruise ships. Except for giardiasis (Chap. 254), parasitic infections are uncommon causes of travelers’ diarrhea in short-term travelers. A growing problem for travelers is the development of antibiotic resistance among many bacterial pathogens. Examples include strains of Campylobacter resistant to quinolones and strains of E. coli, Shigella, and Salmonella resistant to trimethoprim-sulfamethoxazole E. coli. O157 is very rarely a cause of travelers’ diarrhea.
Precautions Some experts think that it is not only what travelers eat but also where they eat that puts them at risk of illness. Food sold by street vendors can carry a high risk, and restaurant hygiene can be a major problem over which the traveler has no control. In addition to discretion in choosing the source of food and water, general precautions include eating foods piping hot; avoiding foods that are raw or poorly cooked; and drinking only boiled or commercially bottled beverages, particularly those that are carbonated. Heating kills diarrhea-causing organisms, whereas freezing does not; therefore, ice cubes made from unpurified water should be avoided. In spite of these recommendations, the literature has repeatedly documented dietary indiscretions by 98% of travelers within the first 72 h after arrival at their destination. The maxim “Boil it, cook it, peel it, or forget it!” is easy to remember but apparently difficult to follow.
Self-Treatment (See also Table 160-5) As travelers’ diarrhea often occurs despite rigorous food and water precautions, travelers should carry medications for self-treatment. An antibiotic is useful in reducing the frequency of bowel movements and the duration of illness in moderate to severe diarrhea. The standard regimen is a 3-day course of a quinolone taken twice daily (or, in the case of some newer formulations, once daily). However, studies have shown that one double dose of a quinolone may be equally effective. For diarrhea acquired in areas such as Thailand, where >90% of Campylobacter infections are quinolone resistant, azithromycin may be a better alternative. Rifaximin, a poorly absorbed rifampin derivative, is highly effective against noninvasive bacterial pathogens such as enterotoxigenic and enteroaggregative E. coli. The current approach to self-treatment of travelers’ diarrhea for the typical short-term traveler is to carry three once-daily doses of an antibiotic and to use as many doses as necessary to resolve the illness. If neither high fever nor blood in the stool accompanies the diarrhea, loperamide should be taken in combination with the antibiotic; studies have shown that this combination is more effective than an antibiotic alone and does not prolong illness.
Prophylaxis Prophylaxis of travelers’ diarrhea with bismuth subsalicylate is widely used but only ~60% effective. For certain individuals (e.g., athletes, persons with a repeated history of travelers’ diarrhea, and persons with chronic diseases), a single daily dose of a quinolone, azithromycin, or rifaximin during travel of <1 month’s duration is 75–90% efficacious in preventing travelers’ diarrhea. Probiotics have been only ~20% effective as prophylaxis. In Europe and Canada, an oral subunit cholera vaccine that cross-protects against enterotoxigenic E. coli (Dukoral) has been shown to provide 30–50% protection against travelers’ diarrhea.
Illness After Return Although extremely common, acute travelers’ diarrhea is usually self-limited or amenable to antibiotic therapy. Persistent bowel problems after the traveler returns home have a less well-defined etiology and may require medical attention from a specialist. Infectious agents (e.g., Giardia lamblia, Cyclospora cayetanensis, Entamoeba histolytica) appear to be responsible for only a small proportion of cases with persistent bowel symptoms. By far the most common causes of persistent diarrhea after travel are postinfectious sequelae such as lactose intolerance and irritable bowel syndrome. A meta-analysis showed that postinfectious irritable bowel syndrome lasting months to years may occur in as many as 4–13% of cases. When no infectious etiology can be identified, a trial of metronidazole therapy for presumed giardiasis, a strict lactose-free diet for 1 week, or a several-week trial of high-dose hydrophilic mucilloid (plus an osmotic laxative such as lactulose or PEG 3350 for persons with alternating diarrhea and constipation) relieves the symptoms of many patients.
PREVENTION OF OTHER TRAVEL-RELATED PROBLEMS
Travelers are at high risk for sexually transmitted diseases (Chap. 163). Surveys have shown that large numbers of travelers engage in casual sex, and there is a reluctance to use condoms consistently. An increasing number of travelers are being diagnosed with illnesses such as schistosomiasis (Chap. 259), dengue (Chap. 233), chikungunya (Chap. 233), and tick-borne rickettsial disease (Chap. 211). Travelers should be cautioned to avoid bathing, swimming, or wading in freshwater lakes, streams, or rivers in parts of northeastern South America, the Caribbean, Africa, and Southeast Asia. Insect repellents are important for prevention not only of malaria but also of other vector-borne diseases. Prevention of travel-associated injury depends mostly on common-sense precautions. Riding on motorcycles (especially without helmets) and in overcrowded public vehicles is not recommended; in developing countries, individuals should never travel by road in rural areas after dark. Of persons who die during travel, fewer than 1% die of infection, whereas 40% die in motor vehicle accidents. Excessive alcohol use has been a significant factor in motor vehicle accidents, drownings, assaults, and injuries. Travelers are cautioned to avoid walking barefoot because of the risk of hookworm and Strongyloides infections (Chap. 257) and snakebites (Chap. 474).
THE TRAVELER’S MEDICAL KIT
A traveler’s medical kit is strongly advisable. The contents may vary widely, depending on the itinerary, duration of stay, style of travel, and local medical facilities. While many medications are available abroad (often over the counter), directions for their use may be nonexistent or in a foreign language, or a product may be outdated or counterfeit. For example, a multicountry study in Southeast Asia showed that a mean of 53% (range, 21–92%) of antimalarial products were counterfeit or contained inadequate amounts of active drug. The sale and marketing of such medications constitute a growing industry. In the medical kit, the short-term traveler should consider carrying an analgesic; an antidiarrheal agent and an antibiotic for self-treatment of travelers’ diarrhea; antihistamines; a laxative; oral rehydration salts; a sunscreen with broad-spectrum protection (UVA and UVB, with the latter at a level of at least 30 SPF); a DEET-containing or equivalent insect repellent for the skin; an insecticide for clothing (permethrin); and, if necessary, an antimalarial drug. To these medications, the long-stay traveler might add a broad-spectrum general-purpose antibiotic (levofloxacin or azithromycin), an antibacterial eye and skin ointment, and a topical antifungal cream. Regardless of the duration of travel, a first-aid kit containing such items as scissors, tweezers, and bandages should be considered. A practical approach to self-treatment of infections in the long-stay traveler who carries a once-daily dose of antibiotics (e.g., levofloxacin) is to use 3 tablets “below the waist” (bowel and bladder infections) and 6 tablets “above the waist” (skin and respiratory infections).
TRAVEL AND SPECIAL HOSTS
PREGNANCY AND TRAVEL
(See also Chap. 8) A woman’s medical history and itinerary, the quality of medical care at her destinations, and her degree of flexibility determine whether travel is wise during pregnancy. According to the American College of Obstetrics and Gynecology, the safest part of pregnancy in which to travel is between 18 and 24 weeks, when there is the least danger of spontaneous abortion or premature labor. Some obstetricians prefer that women stay within a few hundred miles of home after the 28th week of pregnancy in case problems arise. In general, however, healthy women may be advised that it is acceptable to travel.
Relative contraindications to international travel during pregnancy include a history of miscarriage, premature labor, incompetent cervix, or toxemia. General medical problems such as diabetes, heart failure, severe anemia, or a history of thromboembolic disease also should prompt the pregnant woman to postpone her travels. Finally, regions in which the pregnant woman and her fetus may be at excessive risk (e.g., those at high altitudes, those where live-virus vaccines are required, and those where multidrug-resistant malaria is endemic) are not ideal destinations during any trimester.
Malaria Malaria during pregnancy carries a significant risk of morbidity and death. Levels of parasitemia are highest and failure to clear the parasites after treatment is most frequent among primigravidae. Severe disease, with complications such as cerebral malaria, massive hemolysis, and renal failure, is especially likely in pregnancy. Fetal sequelae include spontaneous abortion, stillbirth, preterm delivery, and congenital infection. Chloroquine and mefloquine are considered to be safe in all trimesters.
Enteric Infections Pregnant travelers must be extremely cautious regarding their food and beverage intake. Dehydration due to travelers’ diarrhea can lead to inadequate placental blood flow. Infections such as toxoplasmosis, hepatitis E, and listeriosis also can cause serious sequelae in pregnancy.
The mainstay of therapy for travelers’ diarrhea is rehydration. Loperamide may be used if necessary. For self-treatment, azithromycin may be the best option. Although quinolones are increasingly being used safely during pregnancy and rifaximin is poorly absorbed from the gastrointestinal tract, these drugs are not approved for this indication.
Because of the serious problems encountered when infants are given local foods and beverages, women are strongly encouraged to breast-feed when traveling with a neonate. A nursing mother with travelers’ diarrhea should not stop breast-feeding but should increase her fluid intake.
Air Travel and High-Altitude Destinations Commercial air travel is not a risk to the healthy pregnant woman or to the fetus. The higher radiation levels reported at altitudes of >10,500 m (>35,000 ft) should pose no problem for the healthy pregnant traveler. Since each airline has a policy regarding pregnancy and flying, it is best to check with the specific carrier when booking reservations. Domestic air travel is usually permitted until the 36th week, whereas international air travel is generally curtailed after the 32nd week.
There are no known risks for pregnant women who travel to high-altitude destinations and stay for short periods. However, there are likewise no data on the safety of pregnant women at altitudes of >4500 m (15,000 ft).
THE HIV-INFECTED TRAVELER
(See also Chap. 226) The HIV-infected traveler is at special risk of serious infections due to a number of pathogens that may be more prevalent at travel destinations than at home. However, the degree of risk depends primarily on the state of the immune system at the time of travel. For persons whose CD4+ T cell counts are normal or >500/μL, data suggest no greater risk during travel than for persons without HIV infection. Individuals with AIDS (CD4+ T cell counts of <200/μL) and others who are symptomatic need special counseling and should visit a travel medicine practitioner before departure, especially when traveling to the developing world.
Several countries routinely deny entry to HIV-positive individuals for prolonged stay, even though these restrictions do not appear to decrease rates of transmission of the virus. In general, HIV testing is required for individuals who wish to stay abroad >3 months or who intend to work or study abroad. Some countries will accept an HIV serologic test done within 6 months of departure, whereas others will not accept a blood test done at any time in the traveler’s home country. Border officials often have the authority to make inquiries of individuals entering a country and to check the medications they are carrying. If antiretroviral drugs are identified, the person may be barred from entering the country. Information on testing requirements for specific countries is available from consular offices but is subject to frequent change.
Immunizations All of the HIV-infected traveler’s routine immunizations should be up to date (Chap. 148). The response to immunization may be impaired at CD4+ T cell counts of <200/μL and in some cases at even higher counts. Thus HIV-infected persons should be vaccinated as early as possible to ensure adequate immune responses. For patients receiving antiretroviral therapy, at least 3 months must elapse before regenerated CD4+ T cells can be considered fully functional; therefore, vaccination of these patients should be delayed. However, when the risk of illness is high or the sequelae of illness are serious, immunization is recommended. In certain circumstances, it may be prudent to check the adequacy of the serum antibody response before departure.
Because of the increased risk of infections due to Streptococcus pneumoniae and other bacterial pathogens that cause pneumonia after influenza, the conjugate pneumococcal vaccine (Prevnar 13) followed by the 23-valent polysaccharide vaccine (Pneumovax) as well as influenza vaccine should be administered. The estimated rates of response to influenza vaccine are >80% among persons with asymptomatic HIV infection and <50% among those with AIDS.
In general, live attenuated vaccines are contraindicated for persons with immune dysfunction. Because measles (rubeola) can be a severe or lethal infection in HIV-positive patients, these patients should receive the measles vaccine (or the combination MMR vaccine) unless the CD4+ T cell count is <200/μL. Between 18% and 58% of symptomatic HIV-infected vaccinees develop adequate measles antibody titers, and 50–100% of asymptomatic HIV-infected persons seroconvert.
It is recommended that the live yellow fever vaccine not be given to HIV-infected travelers. Although the potential adverse effects of a live vaccine in an HIV-infected individual are always a consideration, there appear to have been no reported cases of illness in those who have inadvertently received this vaccine. Nonetheless, if the CD4+ T cell count is <200/μL, an alternative itinerary that poses no risk of exposure to yellow fever is recommended. If the traveler is passing through or traveling to an area where the vaccine is required but the disease risk is low, a physician’s waiver should be issued.
A transient increase in HIV viremia (lasting days to weeks) has been demonstrated in HIV-infected individuals after immunization against influenza, pneumococcal infection, and tetanus (Chap. 226). At this point, however, no evidence indicates that this transient increase is detrimental.
Gastrointestinal Illness Decreased levels of gastric acid, abnormal gastrointestinal mucosal immunity, other complications of HIV infection, and medications taken by HIV-infected patients make travelers’ diarrhea especially problematic in these individuals. Travelers’ diarrhea is likely to occur more frequently, to be more severe, to be accompanied by bacteremia, and to be more difficult to treat. Cryptosporidium, Isospora belli, and Microsporidium infections, although uncommon, are associated with increased morbidity and mortality rates in AIDS patients.
The HIV-infected traveler must be careful to consume only appropriately prepared foods and beverages and may benefit from antibiotic prophylaxis for travelers’ diarrhea. Sulfonamides (as used to prevent pneumocystosis) are ineffective because of widespread resistance.
Other Travel-Related Infections Data are lacking on the severity of many vector-borne diseases in HIV-infected individuals. Malaria is especially severe in asplenic persons and in those with AIDS. The HIV load doubles during malaria, with subsidence in ~8–9 weeks; the significance of this increase in viral load is unknown.
Visceral leishmaniasis (Chap. 251) has been reported in numerous HIV-infected travelers. Diagnosis may be difficult, given that splenomegaly and hyperglobulinemia are often lacking and serologic results are frequently negative. Sandfly bites may be prevented by evening use of insect repellents.
Certain respiratory illnesses, such as histoplasmosis and coccidioidomycosis, cause greater morbidity and mortality among patients with AIDS. Although tuberculosis is common among HIV-infected persons (especially in developing countries), its acquisition by the short-term HIV-infected traveler has not been reported as a major problem. From a prospective study, it is estimated that for travelers not engaged in health care the risk of tuberculosis infection is ~3% per year of travel.
Medications Adverse events due to medications and drug interactions are common and raise complex issues for HIV-infected persons. Rates of cutaneous reaction (e.g., increased cutaneous sensitivity to sulfonamides) are unusually high among patients with AIDS. Since zidovudine is metabolized by hepatic glucuronidation, inhibitors of this process may elevate serum levels of the drug. Concomitant administration of the antimalarial drug mefloquine and the antiretroviral agent ritonavir may result in decreased plasma levels of ritonavir; mefloquine may also interact with many of the other protease inhibitors. In contrast, no significant influence of concomitant mefloquine administration on plasma levels of indinavir or nelfinavir was detected in two HIV-infected travelers. Serum levels of mefloquine may be lowered with the use of efavirenz or nevirapine. There are also potential interactions between atovaquone-proguanil (Malarone) and many of the protease inhibitors as well as between Malarone and the nonnucleoside reverse transcriptase inhibitors (NNRTIs). Because of the increase in antiretroviral agents and the lack of accumulated data on their interactions with antimalarial agents, decisions about malaria chemoprophylaxis continue to be difficult; with a short duration of travel, an interaction may be inconsequential. However, doxycycline appears to have no clinically significant interactions with either the protease inhibitors or the NNRTIs. With regard to malaria treatment, a great hypothetical concern is that the antimalarial drugs lumefantrine (combined with artemisinin in Coartem) and halofantrine may interact with HIV protease inhibitors and NNRTIs since drugs in the latter two categories are known to be potent inhibitors of cytochrome P450. In keeping current with antiretroviral drug interactions, a website from the University of Liverpool (www.hiv-druginteractions.org) is helpful.
CHRONIC ILLNESS, DISABILITY, AND TRAVEL
Chronic health problems need not prevent travel, but special measures can make the journey safer and more comfortable.
Heart Disease Cardiovascular events are the main cause of deaths among travelers and of in-flight emergencies on commercial aircraft. Extra supplies of all medications should be kept in carry-on luggage, along with a copy of a recent electrocardiogram and the name and telephone number of the traveler’s physician at home. Pacemakers are not affected by airport security devices, although electronic telephone checks of pacemaker function cannot be transmitted by international satellites. Travelers with electronic defibrillators should carry a note to that effect and ask for hand screening. A traveler may benefit from supplemental oxygen; since oxygen delivery systems are not standard, supplementary oxygen should be ordered by the traveler’s physician well before flight time. Travelers may benefit from aisle seating and should walk, perform stretching and flexing exercises, consider wearing support hose, and remain hydrated during the flight to prevent venous thrombosis and pulmonary embolism.
Chronic Lung Disease Chronic obstructive pulmonary disease is one of the most common diagnoses in patients who require emergency-department evaluation for symptoms occurring during airline flights. The best predictor of the development of in-flight problems is the sea-level PaO2. A PaO2 of at least 72 mmHg corresponds to an in-flight arterial PaO2 of ~55 mmHg when the cabin is pressurized to 2500 m (8000 ft). If the traveler’s baseline PaO2 is <72 mmHg, the provision of supplemental oxygen should be considered. Contraindications to flight include active bronchospasm, lower respiratory infection, lower-limb deep-vein phlebitis, pulmonary hypertension, and recent thoracic surgery (within the preceding 3 weeks) or pneumothorax. Decreased outdoor activity at the destination should be considered if air pollution is excessive.
Diabetes Mellitus Alterations in glucose control and changes in insulin requirements are common problems among patients with diabetes who travel. Changes in time zone, in the amount and timing of food intake, and in physical activity demand vigilant assessment of metabolic control. Because of the risk of foot ulcers, travelers should wear closed footwear that has been proven to be comfortable. The traveler with diabetes should pack medication (including a bottle of regular insulin for emergencies), insulin syringes and needles, equipment and supplies for glucose monitoring, and snacks in carry-on luggage. Insulin is stable for ~3 months at room temperature but should be kept as cool as possible. The name and telephone number of the home physician and a card and bracelet listing the patient’s medical problems and the type and dose of insulin used should accompany the traveler. In order to facilitate international border crossings, travelers should carry a physician’s letter authorizing the carriage of needles and syringes. In traveling eastward (e.g., from the United States to Europe), the morning insulin dose on arrival may need to be decreased. The blood glucose can then be checked during the day to determine whether additional insulin is required. For flights westward, with lengthening of the day, an additional dose of regular insulin may be required.
Other Special Groups Other groups for whom special travel measures are encouraged include patients undergoing dialysis, those with transplants, and those with other disabilities. Up to 13% of travelers have some disability, but few advocacy groups and tour companies dedicate themselves to this growing population. Medication interactions are a source of serious concern for these travelers, and appropriate medical information should be carried, along with the home physician’s name and telephone number. Some travelers taking glucocorticoids carry stress doses in case they become ill. Immunization of these immunocompromised travelers may result in less than adequate protection. Thus the traveler and the physician must carefully consider which destinations are appropriate.
TRAVEL HEALTH INSURANCE
Today, more elderly or chronically ill individuals travel and more of these individuals journey to remote locations and enjoy adventurous activities. Illness or injury abroad is not uncommon and is best considered before the journey. Persons who develop health problems abroad may incur enormous out-of-pocket expenses. Thus prospective travelers should consider purchasing additional travel health insurance and should check with their health insurance company regarding whether they have coverage for illness or injury overseas. Unfortunately, many insurance companies will not cover pre-existing illness if it is the reason for trip cancellation or illness abroad. Most countries do not accept routine health insurance from other countries unless there is a special traveler supplement. In most circumstances, travelers are asked to pay in cash for services rendered on an emergency basis, whether in a physician’s office, in an emergency or urgent care center, or even in a hospital. There are several types of travel insurance. It is wise to purchase trip cancellation insurance, especially, for example, if the traveler has an underlying chronic illness and may need to cancel a trip due to an exacerbation of disease. Travel health insurance will cover expenses in the event that medical care abroad is needed. Evacuation insurance will cover medical evacuation, usually to a medical center in another location where it is deemed that the care is similar to that available in the traveler’s home country. The cost of medical evacuation can easily exceed $100,000 US. There are a number of travel insurance providers, and it is very important to read the fine print carefully and to determine exactly what each company provides, thereby ensuring an appropriate fit for the individual’s particular circumstances. The U.S. Department of State website lists travel health insurance companies (http://travel.state.gov/travel/tips/emergencies/emergencies_5981.html).
MEDICAL TOURISM
Travel for the purpose of obtaining health care abroad has received a great deal of attention in the medical literature and the media. According to the annual U.S. Department of Commerce In-Flight Survey, there were ~500,000 overseas trips during 2006 in which health treatment was at least one purpose of travel. Lower cost is usually cited as the motivation for this type of tourism, and an entire industry has flourished as a result of this phenomenon. However, the quality of facilities, assistance services, and care is neither uniform nor regulated; thus, in most instances, responsibility for assessing the suitability of an individual program or facility lies solely with the traveler. Persons considering this option must recognize that they are almost always at a disadvantage when being treated in a foreign country, particularly if there are complications. Concerns to be addressed include the quality of the health care facility and its staff; language and cultural differences that may impede accurate interpretation of both verbal and nonverbal communication; religious and ethical differences that may be encountered over issues such as efforts to preserve life and limb or the provision of care for the terminally ill; lack of familiarity with the local medical system; limited access of the care provider to the patient’s medical history; the use of unfamiliar drugs and medicines; the relative difficulty of arranging follow-up care back in the United States; and the possibility that such follow-up care may be fraught with problems should there be complications. If serious issues arise, legal recourse may be difficult or impossible. Patients planning to travel abroad to obtain health care, particularly when surgery is involved, should be immunized for hepatitis B and should consider having baseline hepatitis C and HIV tests preoperatively. Prevalence rates of hepatitis B and C and HIV infection vary considerably around the world and are generally higher in developing regions than in the United States and Western Europe. The latest information available on the safety of the blood supply outside the United States is the World Health Organization’s Global Database on Blood Safety based on data from 2011 (www.who.int/bloodsafety/global_database/en). Persons researching the accreditation status of overseas facilities should note that, although these facilities may be part of a chain, they are surveyed and accredited individually. Accreditation resources include (1) the Joint Commission International (www.jointcommissioninternational.org), (2) the Australian Council for Healthcare Standards International (www.achs.org.au/achs-international/), and (3) the Canadian Council on Health Services (www.cchsa.ca). The American Medical Association also offers guidelines for medical tourism (www.ama-assn.org/ama1/pub/upload/mm/31/medicaltourism.pdf).
PROBLEMS AFTER RETURN
The most common medical problems encountered by travelers after their return home are diarrhea, fever, respiratory illnesses, and skin diseases (Fig. 149-2). Frequently ignored problems are fatigue and emotional stress, especially in long-stay travelers. The approach to diagnosis requires some knowledge of geographic medicine, in particular the epidemiology and clinical presentation of infectious disorders. A geographic history should focus on the traveler’s exact itinerary, including dates of arrival and departure; exposure history (food indiscretions, drinking-water sources, freshwater contact, sexual activity, animal contact, insect bites); location and style of travel (urban vs. rural, first-class hotel accommodation vs. camping); immunization history; and use of antimalarial chemosuppression. Recently, some travelers who have been hospitalized abroad have been shown on return to be colonized with multidrug-resistant bacteria such as Enterobacteriaceae producing extended-spectrum β-lactamases and bacteria producing NDM-1 (New Delhi metallo-β-lactamase 1).
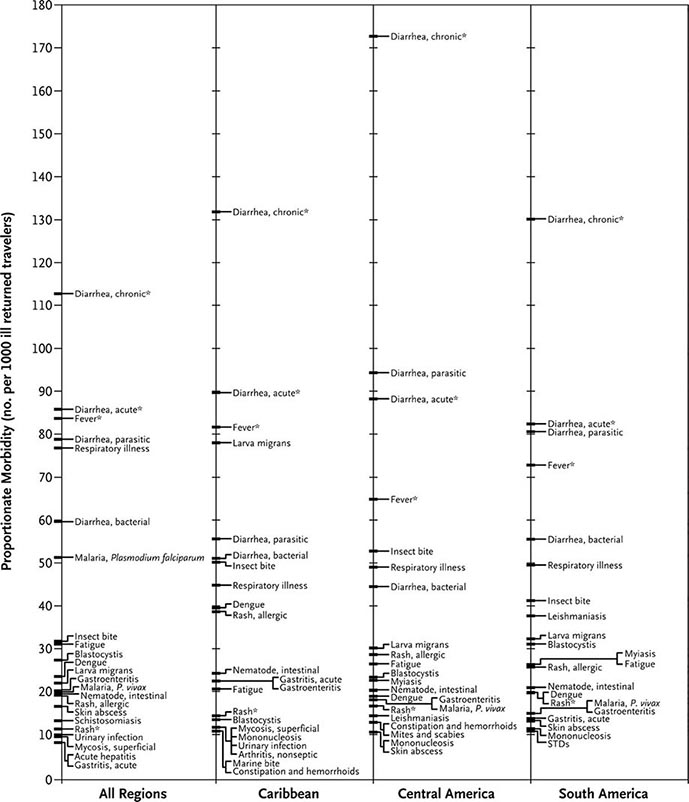
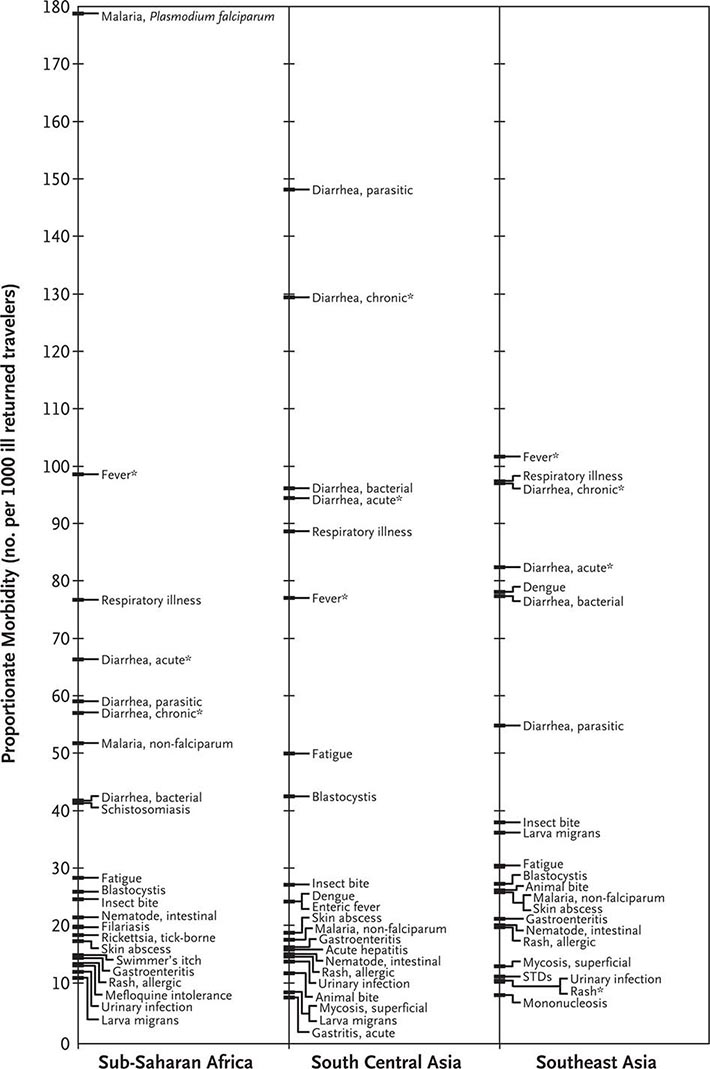
FIGURE 149-2 Proportionate morbidity among ill travelers returning from the developing world, according to region of travel. The proportions (not incidence rates) are shown for each of the top 22 specific diagnoses among all ill returned travelers within each region. STDs, sexually transmitted diseases. Asterisks indicate syndromic diagnoses for which specific etiologies could not be assigned. (Reprinted from DO Freedman et al: N Engl J Med 354:119, 2006.)
DIARRHEA
See “Prevention of Gastrointestinal Illness,” above.
FEVER
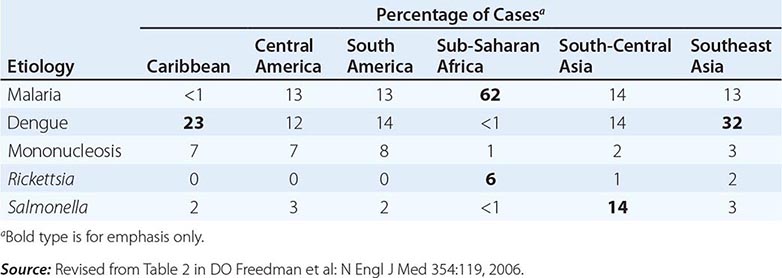
Fever in a traveler who has returned from a malarious area should be considered a medical emergency because death from P. falciparum malaria can follow an illness of only several days’ duration. Although “fever from the tropics” does not always have a tropical cause, malaria should be the first diagnosis considered. The risk of P. falciparum malaria is highest among travelers returning from Africa or Oceania and among those who become symptomatic within the first 2 months after return. Other important causes of fever after travel include viral hepatitis (A and E), typhoid and paratyphoid fever, bacterial enteritis, arboviral infections (e.g., dengue fever), rickettsial infections (including tick typhus, scrub typhus, and Q fever), and—in rare instances—leptospirosis, acute HIV infection, and amebic liver abscess. A cooperative study by GeoSentinel (an emerging infectious disease surveillance group established by the CDC and the International Society of Travel Medicine) showed that, among 3907 febrile returned travelers, malaria was acquired most often in Africa, dengue in Southeast Asia and the Caribbean, typhoid fever in southern Asia, and rickettsial infections (tick typhus) in South Africa (Table 149-3). Outbreaks of dengue, previously considered to be very rare in Africa, have been documented recently in Angola, Kenya, and Tanzania. However, in at least 25% of cases, no etiology of the fever can be found and it resolves spontaneously. Clinicians should keep in mind that no present-day antimalarial agent guarantees protection from malaria and that some immunizations (notably, that against typhoid fever) are only partially protective.
ETIOLOGY AND GEOGRAPHIC DISTRIBUTION OF SYSTEMIC FEBRILE ILLNESS IN RETURNED TRAVELERS (N = 3907) |
When no specific diagnosis is forthcoming, the following investigations, where applicable, are suggested: complete blood count, liver function tests, thick/thin blood films or rapid diagnostic testing for malaria (repeated several times if necessary), urinalysis, urine and blood cultures (repeated once), chest x-ray, and collection of an acute-phase serum sample to be held for subsequent examination along with a paired convalescent-phase serum sample.
SKIN DISEASES
Pyodermas, sunburn, insect bites, skin ulcers, and cutaneous larva migrans are the most common skin conditions affecting travelers after their return home. In those with persistent skin ulcers, a diagnosis of cutaneous leishmaniasis, mycobacterial infection, or fungal infection should be considered. Careful, complete inspection of the skin is important in detecting the rickettsial eschar in a febrile patient or the central breathing hole in a “boil” due to myiasis.
EMERGING INFECTIOUS DISEASES
In recent years, travel and commerce have fostered the worldwide spread of HIV infection, led to the reemergence of cholera as a global health threat, and created considerable fear about the possible spread of novel respiratory diseases, including those caused by influenza viruses (H5N1, H1N1, and H7N9). For travelers, there are more common, everyday concerns. One of the largest outbreaks of dengue fever ever documented is now raging in Latin America and Southeast Asia; chikungunya virus has spread rapidly from Africa to southern Asia, southern Europe, and, for the first time in the Western Hemisphere, the Caribbean; schistosomiasis is being described in previously unaffected lakes in Africa; and antibiotic-resistant strains of sexually transmitted and enteric pathogens are emerging at an alarming rate in the developing world. In addition, concerns have been raised about the potential for bioterrorism involving not only standard strains of unusual agents but mutant strains as well.
CONCLUSIONS
The growth of global travel and migration now demand that the clinician become as familiar as possible with travel medicine. Practitioners may choose either to refer their patients to a travel clinic before departure or to acquire knowledge that enables them to provide pretravel counseling and to prescribe appropriate vaccinations and chemoprophylaxis. It is equally important for physicians seeing ill returned travelers to be familiar with common post-travel syndromes and diseases, particularly those that may have been acquired in the developing world, and to identify other physicians who can assist with complex post-travel illnesses. The CDC publishes a biennial text, Health Information for International Travel (accessed through their website at www.cdc.gov/travel) that provides pretravel health recommendations. The International Society of Travel Medicine (www.istm.org) publishes a list of travel clinics, and the American Society of Tropical Medicine and Hygiene (www.astmh.org) publishes a list of clinical tropical medicine specialists.
As Nobel Laureate Dr. Joshua Lederberg pointed out, “The microbe that felled one child in a distant continent yesterday can reach yours today and seed a global pandemic tomorrow.” The vigilant clinician understands that the importance of a thorough travel history cannot be overemphasized.
150e | Laboratory Diagnosis of Infectious Diseases |
The laboratory diagnosis of infection requires the demonstration—either direct or indirect—of viral, bacterial, fungal, or parasitic agents in tissues, fluids, or excreta of the host. Clinical microbiology laboratories are responsible for processing these specimens and also for determining the antibiotic susceptibility of bacterial and fungal pathogens. Traditionally, detection of pathogenic agents has relied largely on either the microscopic visualization of pathogens in clinical material or the growth of microorganisms in the laboratory. Identification generally is based on phenotypic characteristics such as fermentation profiles for bacteria, cytopathic effects in tissue culture for viral agents, and microscopic morphology for fungi and parasites. These techniques are reliable but are often time-consuming. Increasingly, the use of nucleic acid probes is becoming a standard method for detection, quantitation, and/or identification in the clinical microbiology laboratory, gradually replacing phenotypic characterization and microscopic visualization methods. This chapter discusses general concepts of diagnostic testing, with an emphasis on detection of bacteria. Detection of viral, fungal, and parasitic pathogens is discussed in greater detail in separate chapters (see Chaps. 214e, 235, and 245e, respectively).
DETECTION METHODS
Reappraisal of the methods employed in the clinical microbiology laboratory has led to the development of strategies for detection of pathogenic agents through nonvisual biologic signal detection systems. A biologic signal is generated by detection of a material that can be reproducibly differentiated from other substances present in the sample. Key issues in the use of a biologic signal are distinguishing it from background noise and translating it into meaningful information. Examples of useful materials for detection of biologic signals applicable to clinical microbiology include structural components of bacteria, fungi, and viruses; specific antigens; metabolic end products; unique DNA or RNA base sequences; enzymes; toxins or other proteins; and surface polysaccharides.
A detector is used to sense a signal and discriminate between that signal and background noise. Detection systems range from the trained eyes of a technologist assessing morphologic variations to electronic instruments such as gas-liquid chromatographs or mass spectrometers. The sensitivity with which signals can be detected varies widely. It is essential to use a detection system that discerns small amounts of signal even when biologic background noise is present—i.e., that is both sensitive and specific. Common detection systems include immunofluorescence; chemiluminescence for DNA/RNA probes; flame ionization detection of short- or long-chain fatty acids; and detection of substrate utilization or end-product formation as color changes, of enzyme activity as a change in light absorbance, of turbidity changes as a measure of growth, of cytopathic effects in cell lines, and of particle agglutination as a measure of antigen presence.
Amplification enhances the sensitivity with which weak signals can be detected. The most common microbiologic amplification technique is growth of a single bacterium into a discrete, visible colony on an agar plate or into a suspension containing many identical organisms. The advantage of growth as an amplification method is that it requires only an appropriate growth medium; the disadvantage is the amount of time required. More rapid amplification of biologic signals can be achieved with techniques such as polymerase chain reaction (PCR), ligase chain reaction (LCR), and transcription-mediated amplification (TMA), all of which target the pathogen’s DNA/RNA; enzyme immunoassays (EIAs) for antigens and antibodies; electronic amplification (for gas-liquid chromatography assays); antibody capture methods (for concentration and/or separation); and selective filtration or centrifugation.
DIRECT DETECTION
Direct detection refers to detection of pathogens without the use of culture. Molecular methods of direct detection are discussed below.
MICROSCOPY AND STAINING
The field of microbiology was defined largely by the development and use of the microscope. The examination of specimens by microscopic methods rapidly provides useful diagnostic information. Staining techniques permit organisms to be seen more clearly.
The simplest method for microscopic evaluation is the wet mount, which is used, for example, to examine cerebrospinal fluid (CSF) for the presence of Cryptococcus neoformans, with India ink as a background against which to visualize large-capsuled yeast cells. Wet mounts with dark-field illumination also are used to detect spirochetes in genital lesions and Borrelia or Leptospira in blood. Skin scrapings and hair samples can be examined with the use of either 10% KOH wet-mount preparations or the calcofluor white method and ultraviolet illumination to detect fungal elements as fluorescing structures. Staining of wet mounts—e.g., with lactophenol cotton blue stain for fungal elements—often is used for morphologic identification.
Bacteria are difficult to see by light microscopy unless they are stained. Although simple one-step stains can be used, differential stains are more common.
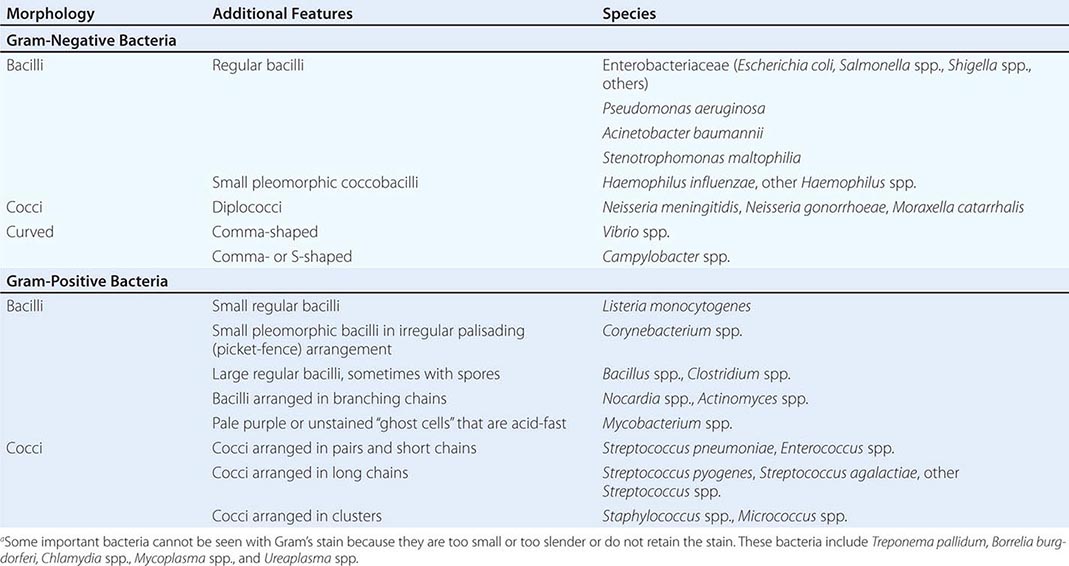
Gram’s Stain Gram’s stain differentiates between organisms with thick peptidoglycan cell walls (gram-positive) and those with thin peptidoglycan cell walls and outer membranes that can be dissolved with alcohol or acetone (gram-negative). Morphology and Gram’s stain characteristics often can be used to categorize stained organisms into groups such as streptococci, staphylococci, and clostridia (Table 150e-1). Gram’s stain is particularly useful for examining sputum for polymorphonuclear leukocytes (PMNs) and bacteria. Sputum specimens from immunocompetent patients with ≥25 PMNs and <10 epithelial cells per low-power field often provide clinically useful information. However, the presence in “sputum” samples of >10 epithelial cells per low-power field and of multiple bacterial types suggests contamination with oral microflora. Despite the difficulty of discriminating between normal microflora and pathogens, Gram’s stain may prove useful for specimens from areas with a large resident microflora if a useful biologic marker (signal) is available. Gram’s staining of vaginal swab specimens can be used to detect epithelial cells covered with gram-positive bacteria in the absence of lactobacilli and the presence of gram-negative rods—a scenario regarded as a sign of bacterial vaginosis. Similarly, examination of stained stool specimens for leukocytes is useful as a screening procedure before testing for Clostridium difficile toxin or other enteric pathogens.
INTERPRETATION OF GRAM’S STAINa |
The examination of samples from normally sterile body sites (e.g., CSF or joint, pleural, or peritoneal fluid) with Gram’s stain is useful for determining whether bacteria and/or PMNs are present. The sensitivity is such that >104 bacteria/mL should be detected. Centrifugation often is performed before staining to concentrate specimens thought to contain low numbers of organisms. This simple method is particularly useful for examination of CSF for bacteria and white blood cells or examination of sputum for mycobacteria.
Acid-Fast Stain The acid-fast stain identifies acid-fast bacteria (AFB; mycobacteria) by their retention of carbol fuchsin dye after acid/organic solvent disruption. Modifications of this procedure allow the differentiation of Actinomyces from Nocardia or other weakly (or partially) acid-fast organisms. The acid-fast stain is applied to sputum, other fluids, and tissue samples when Mycobacterium species are suspected. Because few AFB may be present in an entire smear, even when the specimen has been concentrated by centrifugation, identification of the pink/red AFB against the blue background of the counterstain requires a trained eye. An alternative method for detection of AFB is the auramine-rhodamine fluorescent dye stain.
Fluorochrome Stains Fluorochrome stains such as acridine orange are used to identify white blood cells, yeasts, and bacteria in body fluids. Capsular, flagellar, and spore stains are used for identification or demonstration of characteristic structures.
Immunofluorescent Stains The direct immunofluorescent antibody technique uses antibody coupled to a fluorescent compound (e.g., fluorescein) and directed at a specific antigenic target to visualize organisms. When samples are examined under appropriate conditions, the fluorescing compound absorbs ultraviolet light and re-emits light at a higher wavelength that is visible to the human eye. In the indirect immunofluorescent antibody technique, an unlabeled (target) antibody binds a specific antigen. The specimen is then stained with a fluorochrome-labeled antibody directed at the target antibody. Because each unlabeled target antibody attached to the appropriate antigen has multiple sites for attachment of the second antibody, the visual signal is amplified. Immunofluorescence is used to detect viral antigens (e.g., cytomegalovirus, herpes simplex virus, and respiratory viruses) within cultured cells or clinical specimens as well as many difficult-to-grow bacterial agents (e.g., Legionella pneumophila) in clinical specimens.
MACROSCOPIC ANTIGEN DETECTION
Latex agglutination assays and EIAs are rapid and inexpensive methods for identifying organisms, extracellular toxins, and viral agents by means of protein and polysaccharide antigens. Such assays may be performed directly on clinical samples or after growth of organisms on agar plates or in viral cell cultures. Antibodies coupled to a reporter (such as latex particles or an enzyme) are used for detection of antibody–antigen binding reactions.
Direct agglutination of bacterial cells with specific antibody is simple but relatively insensitive; latex agglutination and EIAs are more sensitive. Some cell-associated antigens, such as capsular polysaccharides and lipopolysaccharides, can be detected by agglutination of a suspension of bacterial cells when antibody is added; this method is useful for typing of the somatic antigens of Shigella and Salmonella. EIAs employ antibodies coupled to an enzyme, and an antigen–antibody reaction results in the conversion of a colorless substrate to a colored product. Most of these assays provide information about whether antigen is present but do not quantify the antigen. EIAs are also useful for detecting bacterial toxins—e.g., toxins produced by Shiga toxin–producing Escherichia coli.
Rapid and simple immunoassays for antigens of group A Streptococcus, influenza virus, and respiratory syncytial virus can be used in the clinical setting without a specialized diagnostic laboratory. Such tests usually are reasonably specific but may have only modest sensitivity.
DETECTION OF PATHOGENIC AGENTS BY SEROLOGIC METHODS
Measurement of serum antibody provides an indirect marker for past or current infection with a specific viral agent or other pathogens, including Brucella, Legionella, Rickettsia, and Helicobacter pylori. Serologic methods can be used to determine whether an individual has protective antibody levels or is infected by a specific pathogen. Determination of an antibody level as a measure of current immunity is important in the case of viral agents for which there are vaccines, such as rubella virus and varicella-zoster virus; assays for this purpose normally use one or two dilutions of serum for a qualitative determination of protective antibody levels. Quantitative serologic assays to detect increases in antibody titers most often employ paired serum samples obtained at the onset of illness and 10–14 days later (i.e., acute- and convalescent-phase samples). Since the incubation period before symptoms are noted may be long enough for an antibody response to occur, the demonstration of acute-phase antibody alone is often insufficient to establish the diagnosis of active infection as opposed to past exposure. A fourfold increase in total antibody titer between the acute- and convalescent-phase samples is regarded as evidence for active infection. In addition, IgM may be useful as a measure of an early, acute-phase antibody response. For certain viral agents, such as Epstein-Barr virus, the antibodies produced may be directed at different antigens during different phases of the infection. For this reason, most laboratories test for antibody directed at both viral capsid antigens and antigens associated with recently infected host cells to determine the stage of infection.
DETECTION OF PATHOGENIC AGENTS BY CULTURE
SPECIMEN COLLECTION AND TRANSPORT
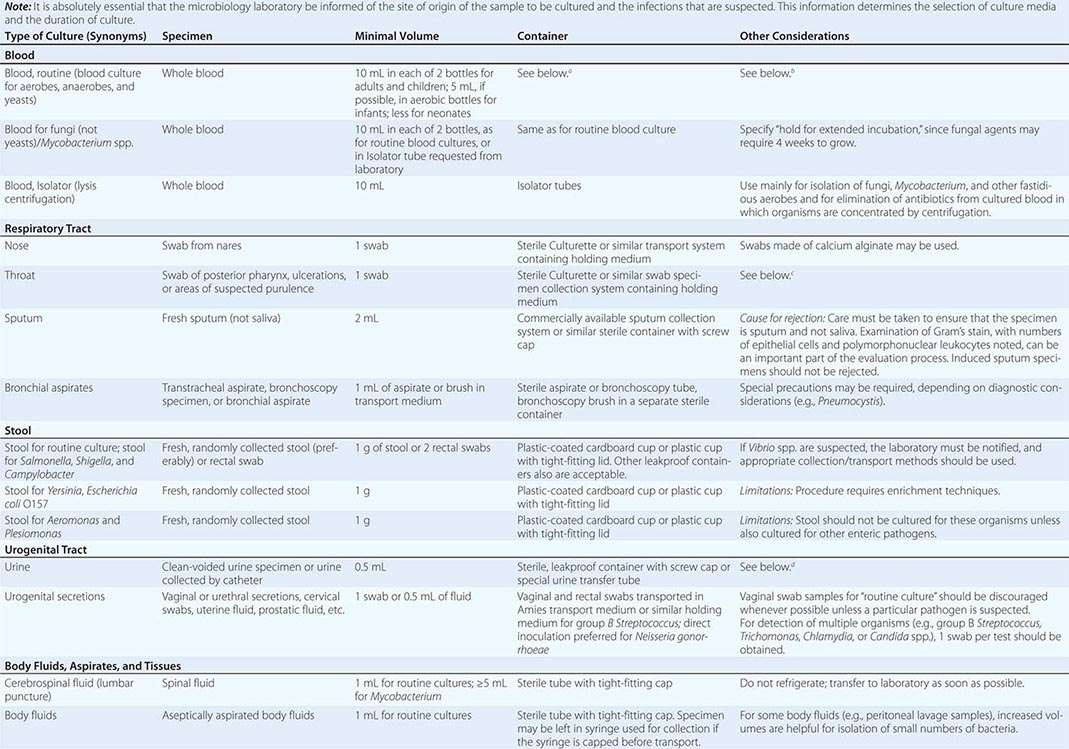
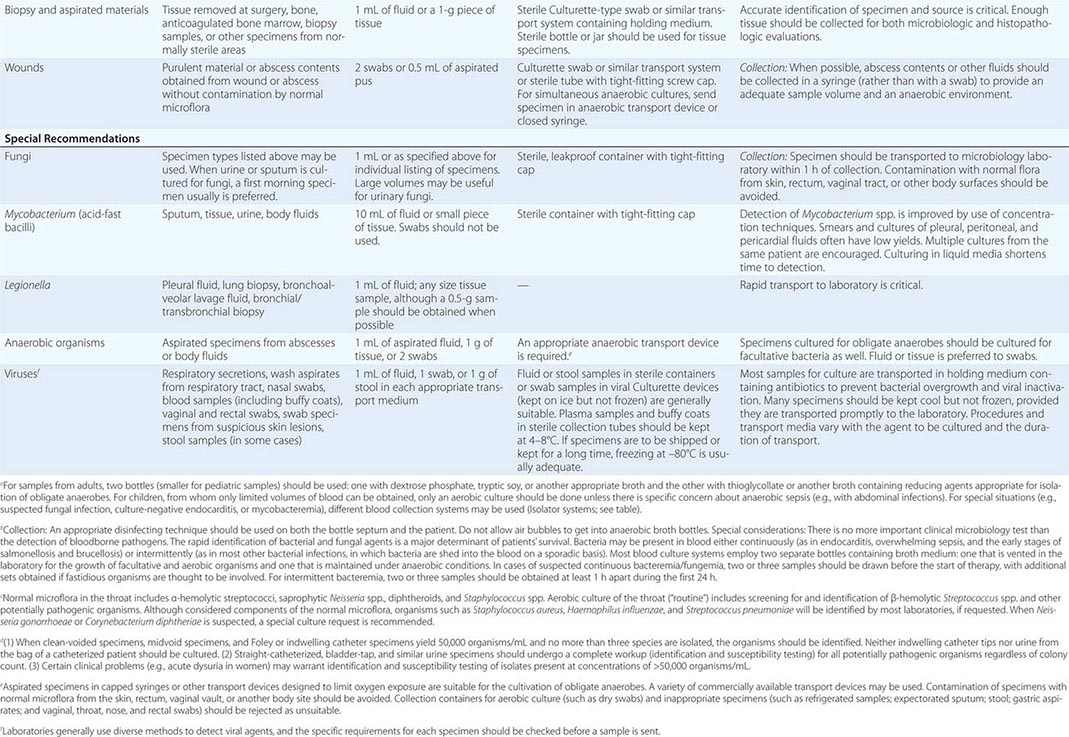
To culture bacterial, fungal, or viral pathogens, an appropriate sample must be placed into the proper medium for growth. The success of efforts to identify a specific pathogen often depends on the collection and transport process coupled to a laboratory-processing algorithm suitable for the specific sample/agent. In some instances, it is better for specimens to be plated at the time of collection rather than first being transported to the laboratory (e.g., urethral swabs being cultured for Neisseria gonorrhoeae). In general, the more rapidly a specimen is plated onto appropriate media, the better the chance is for isolating bacterial pathogens. Deep tissue or fluid (pus) samples are more likely to give useful culture results than are superficial swab specimens. Table 150e-2 lists procedures for collection and transport of common specimens. Because there are many pathogen-specific paradigms for these procedures, it is important to seek advice from the microbiology laboratory when in doubt about a particular situation.
INSTRUCTIONS FOR COLLECTION AND TRANSPORT OF SPECIMENS FOR CULTURE |
ISOLATION OF BACTERIAL PATHOGENS
Isolation of pathogens from clinical material relies on the use of artificial media that support bacterial growth. Such media are composed of agar, nutrients, and sometimes substances that inhibit the growth of other bacteria. Broth is employed for growth of organisms from specimens with few bacteria, such as peritoneal dialysis fluid or CSF, or from samples in which anaerobes or other fastidious organisms may be present. Broths that allow the growth of small numbers of organisms may be subcultured onto solid medium once growth is detected. The use of liquid medium for all specimens is not worthwhile.
Two basic strategies are used to isolate pathogenic bacteria. The first is to employ enriched media that support the growth of any bacteria that may be present at a site that is normally sterile, such as blood or CSF. The second strategy is to use selective media to isolate specific bacterial species from samples that contain many bacteria under normal conditions (e.g., stool or genital tract secretions). Antimicrobial agents or other substances are incorporated into the agar medium to inhibit growth of all but the bacteria of interest. After incubation, organisms that grow on such media are characterized further to determine whether they are pathogens (Fig. 150e-1).
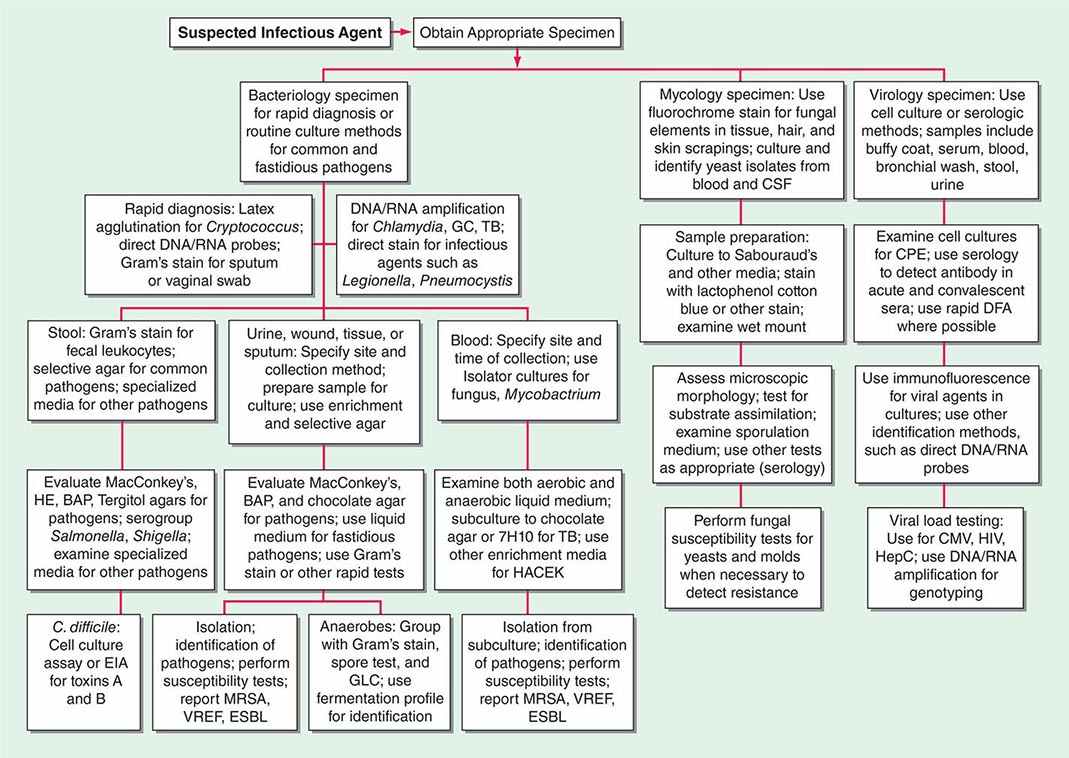
FIGURE 150e-1 Common specimen-processing algorithms used in clinical microbiology laboratories. BAP, blood agar plate; CMV, cytomegalovirus; CPE, cytopathic effects; CSF, cerebrospinal fluid; DFA, direct fluorescent antibody; EIA, enzyme immunoassay; ESBL, extended-spectrum β-lactamase; GBS, group B Streptococcus; GC, Neisseria gonorrhoeae; GLC, gas-liquid chromatography; HACEK, Haemophilus aphrophilus/parainfluenzae/paraphrophilus, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae; HE, Hektoen enteric medium; HepC, hepatitis C virus; HIV, human immunodeficiency virus; MRSA, methicillin-resistant Staphylococcus aureus; TB, Mycobacterium tuberculosis; VREF, vancomycin-resistant Enterococcus faecium.
BLOOD CULTURE
The detection of microbial pathogens in blood is difficult because the number of organisms present in the sample is often low and the organisms’ integrity and ability to replicate may be damaged by humoral defense mechanisms or antimicrobial agents. Automated blood culture systems detect production of gas (mainly CO2) by bacteria or yeasts growing in broth in a blood culture bottle. Because the bottles are monitored frequently, a positive culture often is detected more rapidly than by manual techniques, and important information, including the results of Gram’s stain and preliminary susceptibility assays, can be obtained sooner. Several factors affect the yield of blood culture from bacteremic patients. Increasing the volume of blood tested increases the chance of a positive culture. For example, a sample-size increase from 10 to 20 mL of blood increases the proportion of positive cultures by ~30%, although this effect is less pronounced in patients with bacterial endocarditis. Obtaining multiple samples for culture (up to three per 24-h period) also increases the chance of detecting a bacterial pathogen. Prolonged culture and blind subculture for detection of most fastidious bacteria (e.g., HACEK organisms) are not needed with automated blood culture systems.
Automated systems also have been applied to the detection of microbial growth from specimens other than blood, such as peritoneal and other normally sterile fluids. Mycobacterium species can be detected in certain automated systems if appropriate liquid media are used for culture. Although automated blood culture systems are more sensitive than lysis-centrifugation methods (e.g., Isolator) for yeasts and most bacteria, lysis-centrifugation culture is recommended for filamentous fungi, Histoplasma capsulatum, and some fastidious bacteria (Legionella and Bartonella).
IDENTIFICATION METHODS
Once bacteria are isolated, characteristics that are readily detectable after growth on agar media (colony size, color, hemolytic reactions, odor, microscopic appearance) may suggest a species, but definitive identification requires additional tests. Identification methods include classic biochemical phenotyping, which is still the most common approach, as well as more sophisticated methods such as mass spectrometry, gas chromatography, and nucleic acid tests (see below).
Biochemical Phenotyping Classic biochemical identification of bacteria entails tests for protein or carbohydrate antigens, the production of specific enzymes, the ability to metabolize specific substrates and carbon sources (such as carbohydrates), or the production of certain metabolites. Rapid versions of some of these tests are available, and many common organisms can be identified on the first day of growth. Other organisms, particularly gram-negative bacteria, require more extensive testing, either manual or automated.
Automated systems allow rapid phenotypic identification of bacterial pathogens. Most of these systems are based on biotyping techniques in which isolates are grown on multiple substrates and the reaction pattern is compared with known patterns for various bacterial species. This procedure is relatively fast. Commercially available systems include miniaturized fermentation, coding to simplify recording of results, and probability calculations for the most likely pathogens. If the biotyping approach is automated and the reading process is coupled to computer-based data analysis, rapidly growing organisms (such as Enterobacteriaceae) can be identified within hours of detection on agar plates.
Several systems use substrates for preformed bacterial enzymes for identification within 2–3 h. These systems do not rely on bacterial growth per se to determine whether a substrate has been used. They employ a heavy inoculum in which specific bacterial enzymes are present in amounts sufficient to convert substrate to product rapidly. In addition, some systems use fluorogenic substrate/end-product detection methods to increase sensitivity through signal amplification.
Gas-Liquid Chromatography Gas-liquid chromatography often is used to detect metabolic end products of bacterial fermentation. One common application is identification of short-chain fatty acids produced by obligate anaerobes during glucose fermentation. Because the types and relative concentrations of volatile acids differ among the various genera and species that make up this group of organisms, such information serves as a metabolic fingerprint for a particular isolate.
Gas-liquid chromatography can be coupled to a sophisticated signal-analysis software system for identification and quantitation of long-chain fatty acids (LCFAs) in the outer membranes and cell walls of bacteria and fungi. For any particular species, the types and relative concentrations of LCFAs are distinctive enough to allow differentiation even from closely related species. An organism may be identified definitively within a few hours after detection of growth on appropriate media.
Matrix-Assisted Laser Desorption/Ionization/Time-of-Flight Mass Spectrometry (MALDI-TOF MS) MALDI-TOF MS is a rapid and accurate method for identifying microorganisms by protein analysis. The organism is mixed with a chemical matrix, dried on a target plate, and then pulsed with a laser. The laser ionizes and vaporizes the microbial proteins, which then travel through a charged vacuum chamber to a detector. The time of flight to the detector is measured for the individual proteins, and the resulting pattern (or fingerprint) is compared with a library of known patterns for various microorganisms to identify the test organism.
The primary clinical advantage of MALDI-TOF is that it takes only minutes to identify an organism, whereas several hours are needed for conventional phenotyping. MALDI-TOF is highly accurate for identification of most bacteria and yeasts grown on solid agar or in blood culture broth. Other potential uses of MALDI-TOF include identification of bacteria and yeasts directly from clinical specimens (e.g., urine), detection of β-lactamase activity, and strain typing of bacteria; however, these applications are still under development.
NUCLEIC ACID TESTS
Techniques for the detection and quantitation of specific DNA and RNA base sequences in clinical specimens have become powerful tools for the diagnosis of bacterial, viral, parasitic, and fungal infections. Nucleic acid tests are used for four purposes. First, they are used to detect, and sometimes to quantify, specific pathogens in clinical specimens. Second, such tests are used for identification of organisms (usually bacteria) that are difficult to identify by conventional methods. Third, nucleic acid tests are used to determine whether two or more isolates of the same pathogen are closely related (i.e., whether they belong to the same “clone” or “strain”). Fourth, these tests are used to predict the sensitivity of organisms to chemotherapeutic agents. Current technology encompasses a wide array of methods for amplification and signal detection, some of which have been approved by the U.S. Food and Drug Administration (FDA) for clinical diagnosis.
Use of nucleic acid tests generally involves lysis of intact cells or viruses and denaturation of the DNA or RNA to render it single-stranded. Probe(s) or primer(s) complementary to the pathogen-specific target sequence are hybridized to the target sequence in a solution or on a solid support, depending on the system employed. In situ hybridization of a probe to a target also is possible and allows the use of probes with agents present in tissue specimens. Once the probe(s) or primer(s) have been hybridized to the target (biologic signal), a variety of strategies may be employed to detect, amplify, and/or quantify the target–probe complex (Fig. 150e-2).
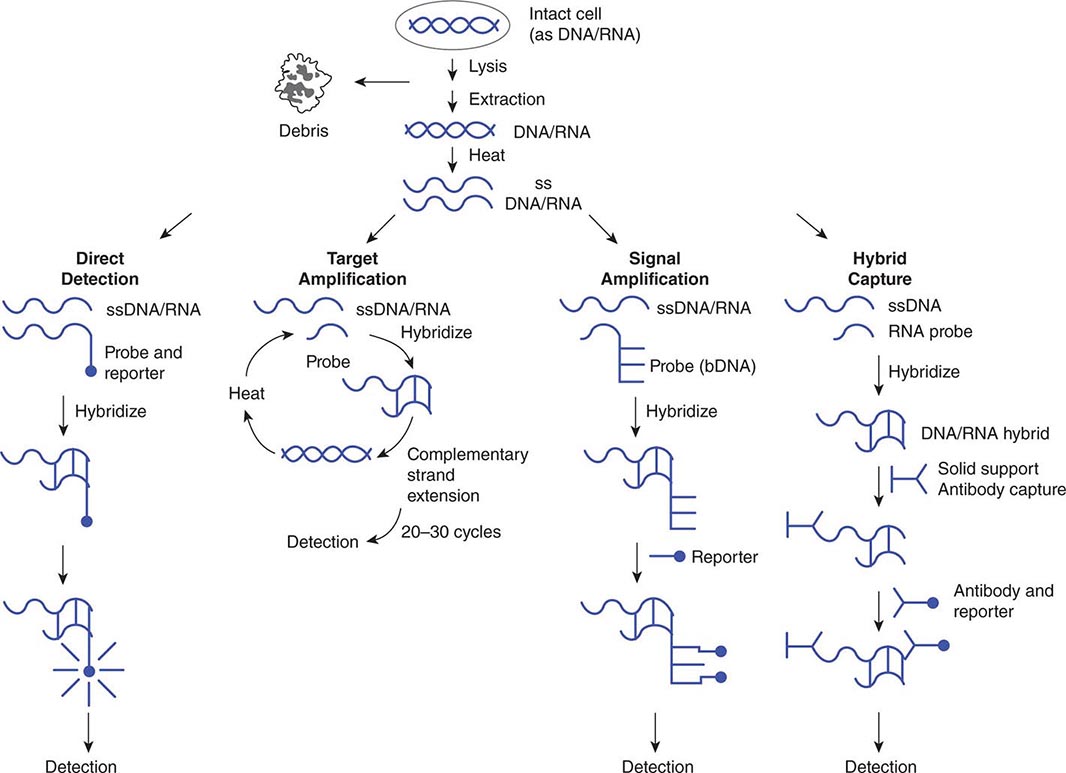
FIGURE 150e-2 Strategies for amplification and/or detection of a target–probe complex. DNA or RNA extracted from microorganisms is heated to create single-stranded (ss) DNA/RNA containing appropriate target sequences. These target sequences may be hybridized directly (direct detection) with probes attached to reporter molecules; they may be amplified by repetitive cycles of complementary strand extension (polymerase chain reaction) before attachment of a reporter probe; or the original target–probe signal may be amplified via hybridization with an additional probe containing multiple copies of a secondary reporter target sequence (branched-chain DNA, or bDNA). DNA/RNA hybrids also can be “captured” on a solid support (hybrid capture), with antibody to the DNA/RNA hybrids used to concentrate them and a second antibody coupled to a reporter molecule attached to the captured hybrid.
PROBES FOR DIRECT DETECTION OF PATHOGENS IN CLINICAL SPECIMENS
Nucleic acid probes are used for direct detection of pathogens in clinical specimens without amplification of the target strand of DNA or RNA. Such tests detect a relatively short sequence of bases specific for a particular pathogen on single-stranded DNA or RNA by hybridization of a complementary sequence of bases (probe) coupled to a reporter system that serves as the signal for detection. Nucleic acid probes are available commercially for direct detection of various bacterial and parasitic pathogens, including Chlamydia trachomatis, N. gonorrhoeae, and group A Streptococcus. A combined assay to detect and differentiate agents of vaginitis/vaginosis (Gardnerella vaginalis, Trichomonas vaginalis, and Candida species) also has been approved. An assortment of probes is available for confirming the identity of cultured pathogens, including some dimorphic molds, Mycobacterium species, and other bacteria (e.g., Campylobacter species, Streptococcus species, and Staphylococcus aureus). Probes for the direct detection of bacterial pathogens often are aimed at highly conserved 16S ribosomal RNA sequences, of which there are many more copies than there are of any single genomic DNA sequence in a bacterial cell. The sensitivity and specificity of probe assays for direct detection are comparable to those of more traditional assays, including EIA and culture.
In an alternative probe assay called hybrid capture, an RNA probe anneals to a DNA target, and the resulting DNA/RNA hybrid is captured on a solid support by antibody specific for DNA/RNA hybrids (concentration/amplification) and detected by chemiluminescent-labeled antibody specific for DNA/RNA hybrids. Hybrid capture assays are available for C. trachomatis, N. gonorrhoeae, and human papillomavirus.
Many laboratories have developed their own probes for pathogens; however, unless a method-validation protocol for diagnostic testing has been performed, federal law in the United States restricts the use of such probes to research.
NUCLEIC ACID AMPLIFICATION TEST (NAAT) STRATEGIES
There are several methods for amplification (copying) of small numbers of molecules of nucleic acid to readily detectable levels. These NAATs include PCR, LCR, strand displacement amplification, and self-sustaining sequence replication. In each case, exponential amplification of a pathogen-specific DNA or RNA sequence depends on primers that anneal to the target sequence. The amplified nucleic acid can be detected after the reaction is complete or (in real-time detection) as amplification proceeds. The sensitivity of NAATs is far greater than that of traditional assay methods such as culture. PCR, the first and still the most common NAAT, requires repeated heating of the DNA to separate the two complementary strands of the double helix, hybridization of a primer sequence to the appropriate target sequence, target amplification using PCR for complementary strand extension, and signal detection via a labeled probe. Methods for the monitoring of PCR after each amplification cycle—via either incorporation of fluorescent dyes into the DNA during primer extension or use of fluorescent probes capable of fluorescence resonance energy transfer—have decreased the time required to detect a specific target. An alternative NAAT employs transcription-mediated amplification, in which an RNA target sequence is converted to DNA, which then is exponentially transcribed into an RNA target. The advantage of this method is that only a single heating/annealing step is required for amplification. Identification of otherwise difficult-to-identify bacteria involves an initial amplification of a highly conserved region of 16S rDNA by PCR. Automated sequencing of several hundred bases is then performed, and the sequence information is compared with large databases containing sequence information for thousands of different organisms. Although 16S sequencing is not as rapid as other methods and is still relatively expensive for routine use in a clinical microbiology laboratory, it is becoming the definitive method for identification of unusual or difficult-to-cultivate organisms.
QUANTITATIVE NUCLEIC ACID TEST STRATEGIES
With the advent of newer therapeutic regimens for HIV-associated disease, cytomegalovirus infection, and hepatitis B and C virus infections, the response to therapy has been monitored by determining both genotype and viral load at various times after treatment initiation. Quantitative NAATs are available for HIV (PCR), cytomegalovirus (PCR), hepatitis B virus (PCR), and hepatitis C virus (PCR and TMA). Many laboratories have validated and perform quantitative assays for these and other pathogens (e.g., Epstein-Barr virus), using analyte-specific reagents for NAATs.
Branched-chain DNA (bDNA) testing is an alternative to NAATs for quantitative nucleic acid testing. In such testing, bDNA attaches to a site different from the target-binding sequence of the original probe. Chemiluminescence-labeled oligonucleotides can then bind to multiple repeating sequences on the bDNA. The amplified bDNA signal is detected by chemiluminescence. bDNA assays for viral load of HIV, hepatitis B virus, and hepatitis C virus have been approved by the FDA. The advantage of bDNA assays over PCR is that only a single heating/annealing step is required to hybridize the target-binding probe to the target sequence for amplification.
APPLICATIONS OF NUCLEIC ACID TESTS
The number of FDA-approved NAATS has increased dramatically and includes tests for Mycobacterium tuberculosis, N. gonorrhoeae, C. trachomatis, group B Streptococcus, and methicillin-resistant S. aureus. FDA-approved multiplex NAAT panels for detection of several respiratory or gastrointestinal pathogens also are available. Again, many laboratories have used commercially available reagents and analyte-specific reagents to create laboratory-developed tests for diagnostic use. Nucleic acid tests are useful to detect and identify difficult-to-grow or noncultivable bacterial pathogens such as Legionella, Ehrlichia, Rickettsia, Babesia, Borrelia, and Tropheryma whipplei. In addition, methods for rapid detection of agents of public health concern, such as Franciscella tularensis, Bacillus anthracis, smallpox virus, and Yersinia pestis, have been developed and are available in regional (state) laboratories and at the Centers for Disease Control and Prevention.
Nucleic acid tests are also used to determine how close the relationship is among different isolates of the same species of pathogen. The demonstration that bacteria of a single clone have infected multiple patients in the context of a possible source of transmission (e.g., a health care provider) offers confirmatory evidence for an outbreak. Pulsed-field gel electrophoresis remains the gold standard for bacterial strain analysis. This method involves the use of restriction enzymes that recognize rare sequences of nucleotides to digest bacterial DNA, resulting in large DNA fragments. These fragments are separated by gel electrophoresis with variable polarity of the electrophoretic current and then are visualized. Similar band patterns (i.e., differences in ≤3 bands) suggest that different bacterial isolates are closely related, or clonal. Simpler methods of strain typing include sequencing of single or multiple genes and PCR-based amplification of repetitive DNA sequences in the bacterial chromosome. Whole bacterial genome sequencing has been used in investigation of some outbreaks, but this method is still under development.
Future applications of nucleic acid testing probably will include the replacement of culture for identification of many pathogens with additional multiplex NAAT and solid-state DNA/RNA chip technology, in which thousands of unique nucleic acid sequences can be detected on a single silicon chip.
SUSCEPTIBILITY TESTING OF BACTERIA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


