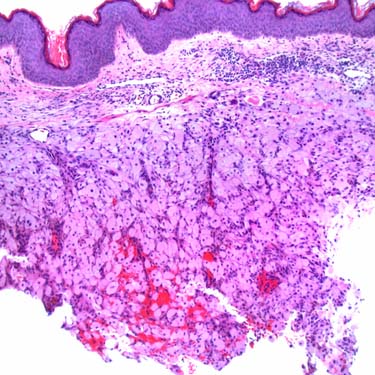
Granular Cell Tumor at Low Magnification Granular cell tumor (GrCT) is a benign tumor of putative Schwann cell origin that occurs in a variety of anatomic sites but shows a predilection for the head and neck region, especially the tongue. This case presented as a dermal nodule on the chest wall, which was clinically suspicious for breast carcinoma.
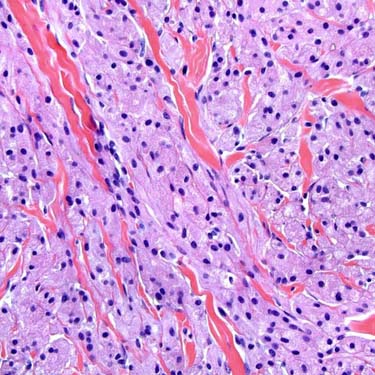
Sheets, Nests, and Cords of Tumor Cells This tumor is composed of sheets, nests, and cords of plump, polygonal cells with abundant eosinophilic granular cytoplasm within a collagenous stroma.
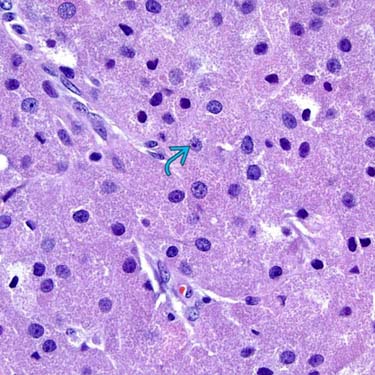
Prominent Granular Cytoplasm Cytologically, the cells of GrCT show prominent, granular cytoplasm, which represents numerous lysosomal structures. Nuclei are generally small and may be dark with dense chromatin or vesicular with a small nucleolus. Occasional scattered larger nuclei and nucleoli may be seen in otherwise benign GrCT.
S100 Immunohistochemistry Strong, diffuse S100 expression is characteristic of GrCT and can help to distinguish it from most entities in its differential diagnosis.
TERMINOLOGY
Abbreviations
• Granular cell tumor (GrCT)
Synonyms
• Granular cell myoblastoma
• Abrikossoff tumor
• Granular cell schwannoma
Definitions
• Benign tumor of putative schwannian origin composed of cells with abundant granular cytoplasm
CLINICAL ISSUES
Epidemiology
• Incidence
Benign GrCT not uncommon
– Malignant GrCT extremely rare
• Age
Any (peak: 40-60 years)
• Sex
Female predilection
• Ethnicity
More prevalent in African Americans
Site
• Wide distribution, usually arises in skin and subcutaneous tissue
Rarely in deep soft tissue sites
• Head and neck region common
Particularly tongue and oral cavity
• Also breast, bronchus, larynx, neurohypophysis, other viscera
• Rarely in nerves, lymph nodes
Presentation
• Usually solitary, slowly growing, painless nodule, plaque, or mass
Multicentric in ~ 10% of cases
– May appear synchronously or metachronously
– May rarely arise in association with Noonan syndrome or LEOPARD syndrome
• Oral cavity/tongue lesions may show concurrent candidiasis



 may be seen in otherwise benign GrCT.
may be seen in otherwise benign GrCT.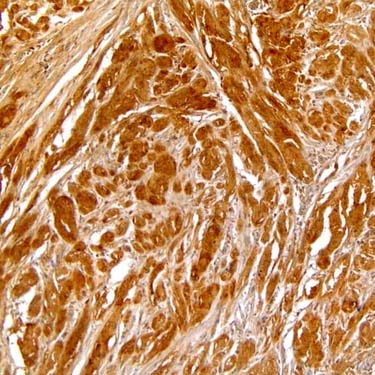
















 Abundant granular, eosinophilic cytoplasm
Abundant granular, eosinophilic cytoplasm





