Patient Story
A 91-year-old woman arrives by ambulance to the emergency department because she was experiencing severe pain in her right middle finger (Figure 100-1). History reveals that she has had swelling of her finger for approximately 1 year. Palpation of the distal interphalangeal joint demonstrated firmness rather than fluctuance. A radiograph of the finger was ordered (Figure 100-2). The radiograph and physical examination are consistent with acute gouty arthritis superimposed on tophaceous gout. The diagnosis was confirmed by an aspirate of the finger that demonstrated negatively birefringent, needle-like crystals, both intracellularly and extracellularly. She was given 1.2 mg of colchicine followed by a second dose of 0.6 mg after 1 hour. Her pain was markedly decreased in 4 hours. Her serum uric acid level was determined to be 10.7 mg/dL. The colchicine was used in this case because the risk of using NSAIDs was considered to be high because of her previous history of gastric bleeding secondary to NSAIDs.

Figure 100-2

This x-ray of the finger in Figure 100-1 shows several tophi (monosodium urate [MSU] deposits) in the soft tissue over the third distal interphalangeal joint. Note the typical punched out lesions under the tophi. This is subchondral bone destruction. (Courtesy of Geiderman JM. An elderly woman with a warm, painful finger. West J Med. 2000;172(1):51-52.)
Introduction
Gout is an inflammatory crystalline arthritis. Elevated uric acid leads to deposition of monosodium urate (MSU) crystals in the joints resulting in a red, hot, swollen joint. Gout typically begins as a monoarthritis, but can become polyarthritic. Treatment of acute episodes include NSAIDs, colchicine, or intraarticular steroids. Chronic therapy includes lowering the uric acid level using dietary modifications and urate-lowering drugs.
Epidemiology
Etiology and Pathophysiology
- Defective uric acid metabolism with inefficient renal urate excretion leads to underexcretion of uric acid and an elevated serum uric acid level.
- Overproduction of uric acid, instead of underexcretion, occurs in approximately 10% of patients with gout, and also leads to elevated serum uric acid levels.
- Elevated serum uric acid leads to deposition of MSU crystals in the joints and the kidneys.
- Crystals trigger proinflammatory cytokines, which cause local inflammation, tissue necrosis, fibrosis, and subchondral bone destruction.
Risk Factors
- Medications that cause hyperuricemia—Thiazide diuretics, cyclosporine, aspirin (<1 g/day).2
- Conditions associated with gout—Insulin resistance, obesity, hypertension, hypertriglyceridemia, hypercholesterolemia, congestive heart failure, renal insufficiency, early menopause, organ transplant.2,3
- Dietary—Increased intake of meat and seafood, alcohol, soft drinks, and fructose.2
Diagnosis
Diagnostic characteristics useful in predicting gout, based on the 1977 criteria developed by the American College of Rheumatology, are:
- Monoarthritis.
- Redness over the joints.
- First metatarsophalangeal (MTP) joint involved (Figure 100-3).
- Unilateral first MTP joint attack.
- Unilateral tarsal joint attack.
- Tophi identified (Figures 100-1, 100-4, and 100-5).
- Hyperuricemia.
- Asymmetric swelling in joint on radiograph.
- Subcortical cysts on radiograph.
- MSU crystals in joint fluid (Figure 100-6).
- Joint fluid culture negative.

Figure 100-4
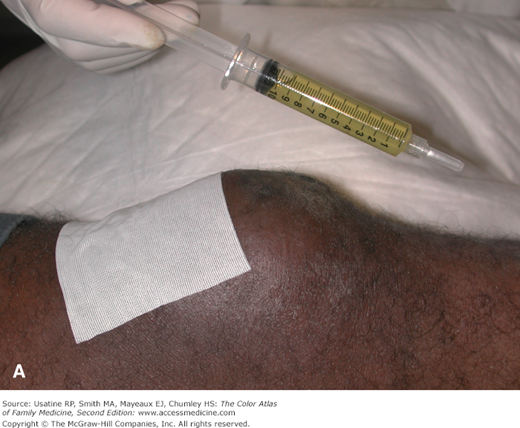
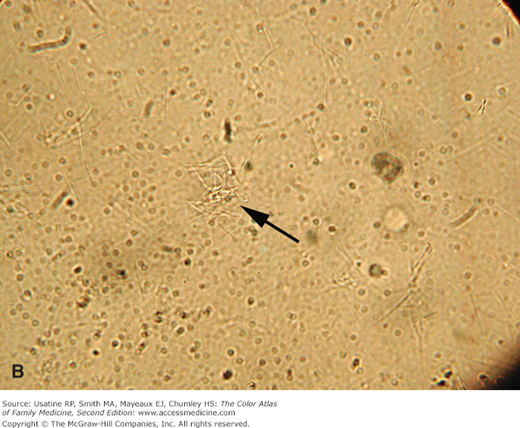
A. A 52-year-old homeless man with acute monoarticular gouty arthritis presenting with knee pain and swelling. Knee aspiration revealed a straw-colored effusion. B. With light microscopy numerous refractile needle-shaped crystals of uric acid were visualized in the joint fluid. The arrow points to a cluster of needle-shaped uric acid crystals. (Reproduced with permission from Usatine RP, Sacks B, Sorci J. A swollen knee. J Fam Pract. 2003;52(1):53-55. Reproduced with permission from Frontline Medical Communications.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


