Patient Story
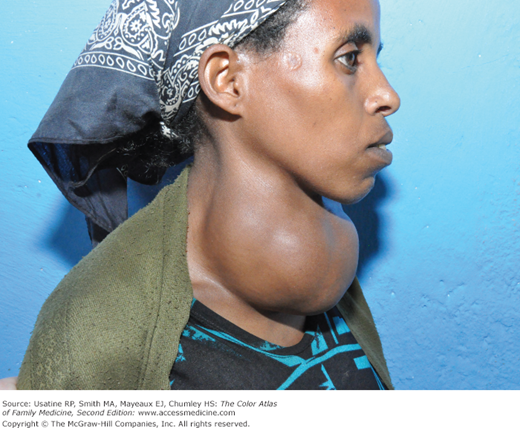
A 55-year-old woman presented with a several-month history of fatigue and weight gain. She reported that she felt puffy and swollen. She had difficulty buttoning the top button of her blouse because her neck was so large, but she reported no neck pain. Review of systems was positive for constipation, dry skin, and cold intolerance. On physical examination, a large goiter was found (Figure 226-1). Laboratory testing revealed an elevated thyroid-stimulating hormone (TSH) and a low free thyroxine (FT4) level confirming hypothyroidism. The patient was started on levothyroxine.

Introduction
- Goiter is a spectrum of changes in the thyroid gland ranging from diffuse enlargement to nodular enlargement depending on the cause. In the United States, the most common etiology of goiter with normal thyroid function or transient dysfunction is thyroiditis.
- Hypothyroidism is a condition caused by lack of thyroid hormone and usually develops as a result of thyroid failure from intrinsic thyroid disease. The most common cause of goitrous hypothyroidism is chronic lymphocytic (Hashimoto) thyroiditis.
- Subclinical thyroid disease refers to a patient with no or minimal thyroid-related symptoms but abnormal laboratory values (elevated TSH and thyroxine level within the normal range).
Epidemiology
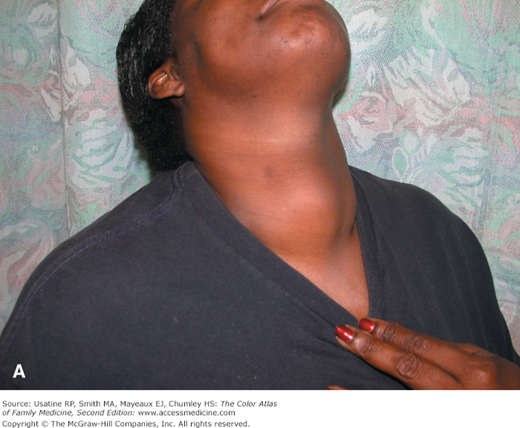
- Worldwide, goiter is the most common endocrine disorder with rates of 4% to 15% in areas of adequate iodine intake and more than 90% where there is iodine deficiency.1 Endemic goiter is defined as goiter that affects more than 5% of the population (Figures 226-2 and 226-3).
- Most goiters are not associated with thyroid dysfunction.
- The prevalence of goitrous hypothyroidism varies from 0.7% to 4% of the population.
- Subclinical hypothyroidism is present in 3% to 10% of population groups and in 10% to 18% of elderly persons.2,3
- The female-to-male ratio of goiter is 3:1, and 6:1 for goitrous hypothyroidism.
- The annual incidence of autoimmune hypothyroidism is 4 in 1000 women and 1 in 1000 men, with a mean age at diagnosis of 60 years.4

Etiology and Pathophysiology
- Iodine deficiency or excess (Figures 226-2 and 226-3).
- TSH stimulation.
- Drugs, including lithium, amiodarone, and α-interferon.
- Autoimmunity/heredity.
Hypothyroidism may be caused by disease of the thyroid gland itself (e.g., Hashimoto thyroiditis), radioiodine thyroid ablation, thyroidectomy, high-dose head and neck radiation therapy, and medications (as above), or, rarely, by pituitary or hypothalamic disorders (e.g., tumors, inflammatory conditions, infiltrative diseases, infections, pituitary surgery, pituitary radiation therapy, and head trauma).2
- Hashimoto thyroiditis is caused by thyroid peroxidase (TPO) antibodies.
- Human leukocyte antigen-D related (HLA-DR) and cytotoxic T-lymphocyte antigen 4 (CTLA-4) are the best-documented genetic risk factors for this disorder.4
- There is marked lymphocytic infiltration of the thyroid in Hashimoto thyroiditis; the infiltrate is composed of activated CD4+ and CD8+ T cells, as well as B cells.
- Thyroid destruction in Hashimoto thyroiditis is believed to be primarily mediated by CD8+ cytotoxic T cells.
Risk Factors
- Symptoms of thyroid hormone deficiency.
- Goiter.
- Personal or family history of thyroid disease.
- Personal treatment of thyroid disease.
- History of autoimmune disease, especially diabetes mellitus.
- High-dose head and neck radiation therapy.
Myxedema coma usually occurs in elderly patients with untreated or inadequately treated hypothyroidism who develop a precipitating event, such as myocardial infarction, stroke, sepsis, or prolonged cold exposure.2
Diagnosis
The history can be the key to the diagnosis:
- A painful neck mass is usually a form of thyroiditis.
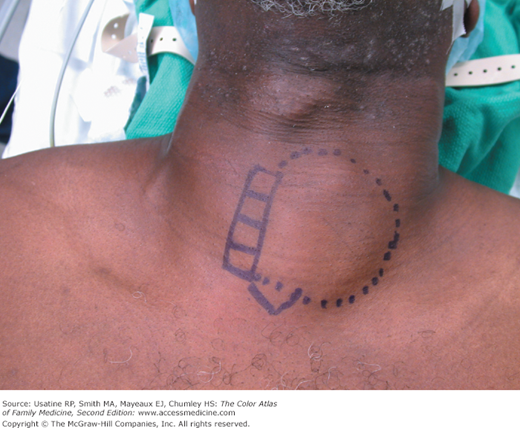
- Large goiters are easily visible before palpating the neck (Figures 226-1, 226-2, 226-3, 226-4, and 226-5).
- Asymmetric goiters can shift the trachea away from the midline (Figure 226-6).


Common signs and symptoms of hypothyroidism are:
- Fatigue and/or weakness.
- Dry and cool skin.
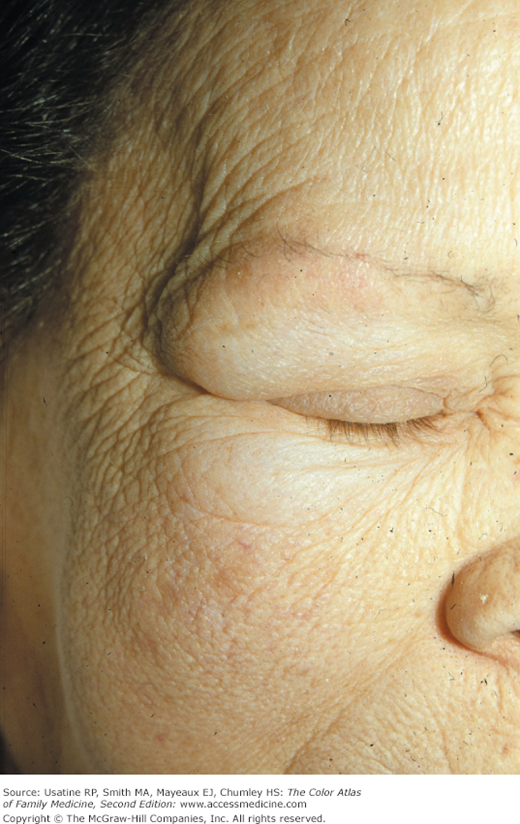
- Diffuse hair loss or thinning of the lateral eyebrows.
- Difficulty concentrating.
- Puffy face/hands/feet from myxedema (Figure 226-7).
- Bradycardia.
- Delayed deep tendon reflex relaxation.
- Weight gain despite poor appetite.
- Constipation.
- The most useful signs for diagnosing hypothyroidism are puffiness (likelihood ratio positive [LR+] 16.2) and delayed ankle reflex (LR+ 11.8).5
Clues to a central cause of hypothyroidism include a history of pituitary/hypothalamic surgery or radiation, headache, visual field defects, or ophthalmoplegia.2
Physical examination maneuvers that help detect goiter are:6
- Neck extension.
- Observation from the side.
- Palpation by locating the isthmus first.
- Having the patient swallow.
- Myxedema coma



