• Negative for desmin, S100, keratin, synaptophysin
Top Differential Diagnoses
• Myopericytoma
• Benign adnexal tumors
• Dermal melanocytic nevus
• Paraganglioma
Clinical Photograph of Subungual Glomangioma This is an example of a subungual glomangioma on the thumb (the nail has been avulsed prior to biopsy ).
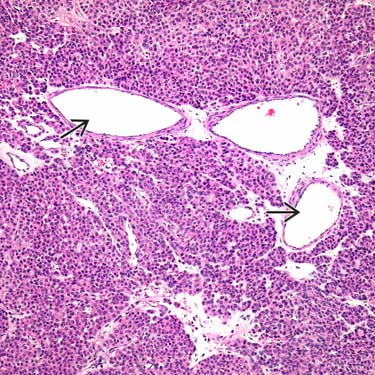
Glomus Tumor at Low Magnification Glomus tumor (GT) is a rare benign tumor that may arise almost anywhere, but shows a predilection for the distal extremities, particularly under the nail bed (subungual). It is histologically characterized by sheets and nests of uniform, round to epithelioid cells arranged around a conspicuous vasculature .
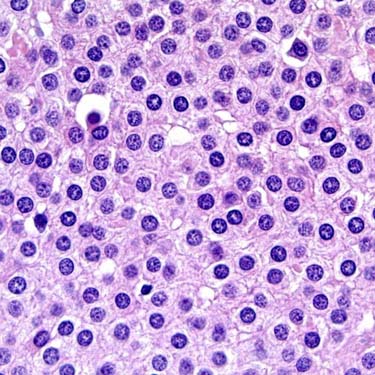
Monotonous Nuclei in Glomus Tumor The distinctive nuclei in GT are strikingly monomorphic and feature a sharply defined, round nuclear contour. They are often described as being “punched out.” Cytoplasmic borders vary in prominence, and may be easy or difficult to visualize, depending upon the individual tumor. Mitotic figures are absent.
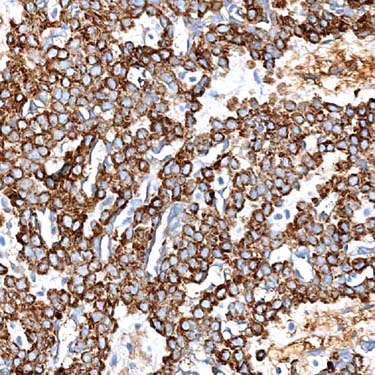
SMA Expression in Glomus Tumor Strong, diffuse cytoplasmic expression of SMA is characteristic of GT. Caldesmon is also typically positive. Desmin is negative.
TERMINOLOGY
Abbreviations
• Glomus tumor (GT)
Definitions
• Perivascular mesenchymal neoplasm composed of cells closely resembling modified smooth muscle cells of normal glomus body
Considered to fall on morphologic spectrum with myopericytoma, myofibroma, and angioleiomyoma
• Several morphologic variants exist, including glomangioma (glomuvenous malformation), glomangiomyoma, glomangiomatosis, and symplastic GT
ETIOLOGY/PATHOGENESIS
Small Subsets Are Inherited
• Often feature multiple lesions
• Multiple familial GT
Inactivation of GLMN gene
• Neurofibromatosis type 1 (NF1)
Biallelic inactivation of NF1 gene
CLINICAL ISSUES
Epidemiology
• Incidence
Rare
– Malignant GT extremely rare
• Age
Most common in young adults (20-40 years)
– Overall wide age range
– Glomangioma variant more common in childhood
• Sex
Female predilection in subungual tumors
Site
• Overall wide distribution
• Most common in distal extremities
Particularly subungual location
• Rarely in other anatomic locations, including visceral organs (particularly GI tract), bone, mediastinum
Presentation
• Typically small, red-blue nodule, often solitary
Multiple in up to 10% of cases
– Multifocality also seen within setting of NF1
• Most arise in skin or subcutis
Rarely in deep soft tissues
• Usually painful
Long history of pain
Pain with exposure to cold &/or tactile stimulation
Treatment
• Complete surgical excision
• Clinical follow-up for malignant GT and GT of uncertain malignant potential
Prognosis
• Excellent prognosis in conventional GT
< 10% recur locally
Includes symplastic forms, glomangiomatosis, and other variants
• Malignant GT is clinically aggressive
Metastases and death of patients in up to 40% of cases
• Large, visceral GT have potential for aggressive behavior regardless of histology
MACROSCOPIC
General Features
• Red-blue nodular lesions
Size
• Most are < 1 cm
Deeper lesions may be larger
MICROSCOPIC
Histologic Features
• Well circumscribed ± fibrous pseudocapsule
Small nests of glomus cells associated with small vessels may be identified around periphery of main tumor
• Typically solid nests of cells within highly vascularized stroma
Vessels range from small to large and ectatic (staghorn appearance)
Tumor cells arranged around vessels, often as cuffs
Diffuse nodular, sheet-like appearance in highly cellular tumors
• Characteristic small, round, uniform tumor cells with pale eosinophilic to amphophilic cytoplasm
Each cell contains single centralized small, round, uniform nucleus
– Sometimes described as “punched out”
– Absence of nuclear atypia and significant mitotic activity
Occasionally cases feature oncocytic or epithelioid cytomorphology
Each cell surrounded by basal lamina
• Hyalinized to myxoid stroma
• No necrosis
• Rare intravascular growth
Only gold members can continue reading. Log In or Register to continue


 ).
).
 .
.