Patient Story
A 45-year-old black man presents with greasy scale over his face and large parts of his chest and back (Figure 205-1). A previous biopsy was diagnostic for Darier disease. His mother has the same condition. His sister has the full-blown disease. His brother has similar nail findings, but his skin is affected only behind the ears (Figure 205-2). The patient has suffered with this condition for his entire life and believes that he has been ostracized from normal social life because of his appearance and bad body odor. He suffers from depression and has used various substances to treat his pain. Topical steroids provide some help for the itching and scaling, but the patient is looking for a more effective treatment. The cost of oral retinoids is currently prohibitive, but an application has been put in for patient assistance to receive acitretin.


Figure 205-2
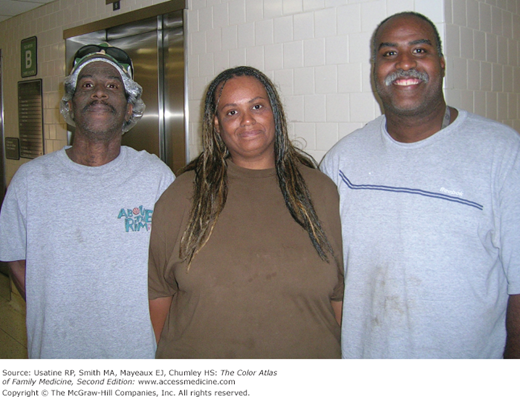
Darier disease present in three siblings. The brother on the left and the sister have the full blown disease. The sister’s face cleared after 3 months of acitretin. The brother on the right has similar nail findings, but his skin is affected only behind the ears. As a family physician, I take care of all three siblings and their mother who also has the disease. (Courtesy of Richard P. Usatine, MD.)
Introduction
There are more than 100 genetic syndromes with cutaneous manifestations that are referred to as genodermatoses. For example, there are disorders of pigmentation (albinism), cornification (the ichthyoses and Darier disease), vascularization (Sturge-Weber syndrome), connective tissue (Ehlers-Danlos syndrome), porphyrin metabolism, other errors of metabolism (phenylketonuria), the immune system (Wiskott-Aldrich syndrome), and DNA repair (ataxia-telangiectasia and xeroderma pigmentosa), to name a few. Some textbooks are dedicated to the topic of genodermatoses alone.1 This chapter introduces the topic and illustrates a couple of genodermatoses. We have chosen two disorders of cornification as an introduction to the genodermatoses: Darier disease and X-linked ichthyosis.
Epidemiology
Etiology and Pathophysiology
- Darier disease—An abnormal calcium pump in the sarco-/endoplasmic reticulum, SERCA2, results from a gene mutation in the ATP2A2 gene. It is inherited in an autosomal-dominant fashion and results in abnormal epidermal differentiation.
- X-linked ichthyosis—A deletion of the steroid sulfatase gene results in keratinocyte retention by inhibiting degradation of the desmosome. It is inherited in an X-linked recessive manner.
Diagnosis
- Clinical features—Greasy, hyperkeratotic, yellowish-brown papules in a seborrheic distribution (Figures 205-1, 205-2, and 205-3). The feet can be covered with hyperkeratotic plaques (Figure 205-4). The palms may have pits or keratotic papules, and the nails can have V-shaped nicking and alternating longitudinal red and white bands (Figure 205-5). The keratotic papules can be intensely malodorous such that it can interfere with normal social situations.
- Typical distribution—The clinical lesions involve skin in the seborrheic distribution (face, ears, scalp, upper chest, upper back, and groin) (Figures 205-1, 205-2, 205-3, and 205-4). The axilla and inframammary areas may be involved (Figure 205-6). In early, mild, or partially treated disease, only the skin behind the ears may be affected (Figure 205-7).2 The nails are characteristically involved.
- Laboratories—Skin biopsy reveals the characteristic histopathology. A test for the ATP2A2 gene mutation can be performed.
Figure 205-3


A. Darier disease with greasy, hyperkeratotic scaling plaques on the face of the 44-year-old woman (sister of the patient in Figure 205-1) with Darier disease prior to her use of acitretin. She is wearing a wig to cover the alopecia and plaques on her scalp. B. Close-up of the hyperkeratotic scaling plaques on the forehead, scalp, and ears. Note the seborrheic distribution. (Courtesy of Richard P. Usatine, MD.)







