Patient Story
A 55-year-old woman presents with a red pruritic area on her face for 3 months (Figure 135-1). The annular distribution immediately is suspicious for a dermatophyte infection. Further investigation demonstrates that the patient has severe tinea pedis in a moccasin distribution. The patient is treated with an oral antifungal agent and her fungal infection clears over the coming month.

Introduction
Fungal infections of the skin and mucous membranes are ubiquitous and common. There are many types of fungus that grow on humans but they all share a predilection for warm and moist areas. Consequently, hot and humid climates promote fungal infections, but many areas of the skin can get warm and sweaty even in cold climates, such as the feet and groin.
Pathophysiology
- Dermatophytes in three genera: Microsporum, Epidermophyton, and Trichophyton. There are approximately 40 species in the three genera and these fungi cause tinea pedis and manus, tinea capitis, tinea corporis, tinea cruris, tinea faciei, and onychomycosis (Figures 135-1 to 135-6).
- Yeasts in the genera of Candida and Pityrosporum (Malassezia)—There are also multiple types of species and the Pityrosporum that cause seborrhea and tinea versicolor (Figures 135-7 and 135-8). Although tinea versicolor has the name tinea in it, it is not a true dermatophyte and may be best called pityriasis versicolor.





Diagnosis
Scaling, erythema, pruritus, central clearing, concentric rings, and maceration (Table 135-1). Changes in pigmentation are not uncommon in various types of tinea especially tinea versicolor.
- Figure 135-1 shows tinea faciei on the face with typical scaling and ring-like pattern, hence, the name ringworm. There is also erythema and central clearing. The patient was experiencing pruritus.
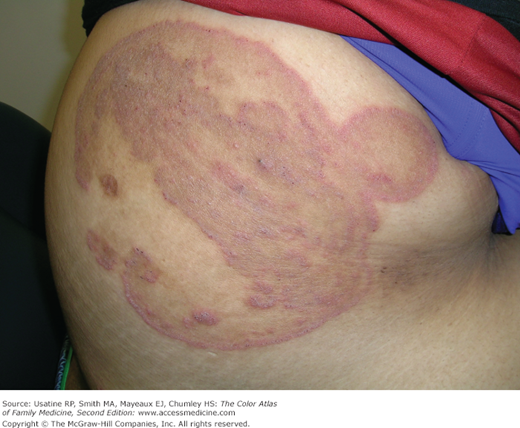
- Figure 135-2 shows annular pruritic lesion with concentric rings in the axilla of a young woman caused by tinea corporis. The concentric rings have a high specificity (80%) for tinea infections.
- Note that tinea infections will not show central clearing in 58% of cases, as in Figure 135-3 in which tinea cruris has no central clearing.
- Post-inflammatory hyperpigmentation is common in skin of color, as seen in Figure 135-4. Note the hyperpigmentation is seen within the area affected by the tinea corporis.
- Hypopigmentation is frequently seen in tinea versicolor (Figure 135-8).
Sign/Symptom | Sensitivity (%) | Specificity (%) | PV+ (%) | PV− (%) | LR+ | LR− |
|---|---|---|---|---|---|---|
Scaling | 77 | 20 | 17 | 80 |



