Patient Story
A 42-year-old woman is seen for multiple papules and pustules on her back (Figure 117-1). Further questioning demonstrates that she was in a friend’s hot tub twice over the previous weekend. The outbreak on her back started after she went into the hot tub the second time. This is a case of Pseudomonas folliculitis or “hot tub” folliculitis. The patient avoided this hot tub and the folliculitis disappeared spontaneously. Another option is to treat with an oral fluoroquinolone that covers Pseudomonas.

Introduction
Epidemiology
- Folliculitis is a cutaneous disorder that affects all age groups and races, and both genders.
- It can be infectious or noninfectious. It is most commonly of bacterial origin (Figures 117-2 and 117-3).
- Pseudofolliculitis or sycosis barbae is most frequently seen in men of color and made worse by shaving (Figure 117-4).1
- Acne keloidalis nuchae or keloidal folliculitis is commonly seen in black patients, but can be seen in patients of any ethnic background (Figures 117-5 and 117-6).2
- Eosinophilic folliculitis is described in patients with HIV infection (Figure 117-7).
- Methicillin-resistant Staphylococcus aureus (MRSA) can pose a challenge to the treatment of folliculitis (Figure 117-8).

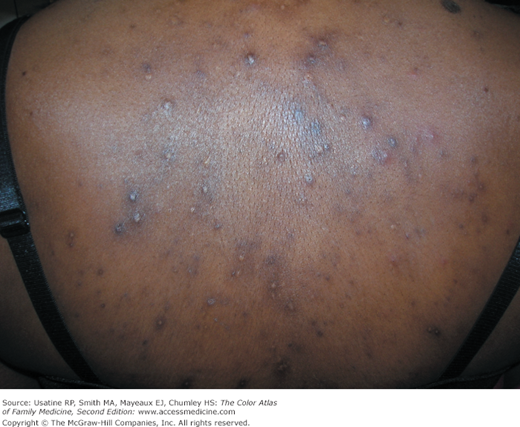




Figure 117-8

MRSA folliculitis in the axilla of a 29-year-old woman. The lesions were present for 4 weeks in the axilla, left forearm, and right thigh. The MRSA was sensitive to tetracyclines and resolved with oral doxycycline. (Courtesy of Alisha N. Plotner, MD, and Robert T. Brodell, MD, and used with permission from Plotner AN, Brodell RT. Bilateral axillary pustules. J Fam Pract. 2008;57(4):253-255. Reproduced with permission from Frontline Medical Communications.)
Etiology and Pathophysiology
- Folliculitis is an infection of the hair follicle and can be superficial, in which it is confined to the upper hair follicle, or deep, in which inflammation spans the entire depth of the follicle.
- Infection can be of bacterial, viral, or fungal origin. S. aureus is by far the most common bacterial causative agent.
- The noninfectious form of folliculitis is often seen in adolescents and young adults who wear tight-fitting clothes. Folliculitis can also be caused by chemical irritants or physical injury.
- Topical steroid use, ointments, lotions, or makeup can swell the opening to the pilosebaceous unit and cause folliculitis.
- Bacterial folliculitis or Staphylococcus folliculitis typically presents as infected pustules most prominent on the face, buttocks, trunk, or extremities. It can progress to a deeper infection with the development of furuncles or boils (Figure 117-9). Infection can occur as a result of mechanical injury or via local spread from nearby infected wounds. An area of desquamation is frequently seen surrounding infected pustules in S. aureus folliculitis.1–3
- Parasitic folliculitis usually occurs as a result of mite infestation (Demodex). These are usually seen on the face, nose, and back and typically cause an eosinophilic pustular-like folliculitis.1
- Folliculitis decalvans is a chronic form of folliculitis involving the scalp, leading to hair loss or alopecia (Figure 117-10). Staphylococci infection is the usual causative agent, but there also has been a suggested genetic component to this condition.1 It is also called tufted folliculitis because some of the hair follicles will have many hairs growing from them simultaneously (Figure 117-11) (see Chapter 189, Scarring Alopecia).
- Acne keloidalis nuchae is a chronic form of folliculitis found on the posterior neck that can be extensive and lead to keloidal tissue and alopecia.1–3 Although it is often thought to occur almost exclusively in black men, it can be seen in men of all ethnic backgrounds and occasionally in women (Figures 117-5 and 117-6) (see Chapter 114, Pseudofolliculitis and Acne Keloidalis Nuchae).
- Fungal folliculitis is epidermal fungal infections that are seen frequently. Tinea capitis infections are a form of dermatophytic folliculitis (see Chapter 137, Tinea Capitis). Pityrosporum folliculitis is caused by yeast infection (Malassezia species) and is seen in a similar distribution as bacterial folliculitis on the back, chest, and shoulders (Figure 117-12) (see Chapter 141, Tinea Versicolor). Candidal infection is less common and is usually seen in individuals who are immunosuppressed, present in hairy areas that are moist, and unlike most cases of folliculitis, may present with systemic signs and symptoms.1–4
- Pseudomonas folliculitis or “hot tub” folliculitis is usually a self- limited infection that follows exposure to water or objects that are contaminated with Pseudomonas aeruginosa (Figure 117-1). This occurs when hot tubs are inadequately chlorinated or brominated. This also occurs when loofah sponges or other items used for bathing become a host for pseudomonal growth. Onset of symptoms is usually within 6 to 72 hours after exposure, with the complete resolution of symptoms in a couple of days, provided that the individual avoids further exposure.4

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


