Feeding Jejunostomy
John Daniel Hunter III
John Roland Porterfield Jr.
DEFINITION
A jejunostomy tube (J-tube) is a flexible soft tube that connects the intraluminal jejunum with the outside world through the abdominal wall. The main function is to provide long-term access to the proximal gastrointestinal (GI) tract for enteral nutrition when oral intake is not possible or inadequate.
A J-tube can be placed through an open or a laparoscopic approach. Often, they are placed in conjunction with a larger operation when it is anticipated that the patient will not progress to adequate oral intake in a timely fashion during the early postoperative course. The J-tube affords the advantage of early enteral nutrition even when the upper GI tract cannot be used.
PATIENT HISTORY AND PHYSICAL FINDINGS
The history and physical exam should focus on the indication for enteral access J-tube, hemodynamic stability of the patient, current functional status of the GI tract, and previous surgeries.
Patients who are hemodynamically unstable generally should not undergo elective J-tube placement. The patient should be assessed for a functional GI tract distal to the ligament of Treitz (LOT) and should not have evidence of mechanical bowel obstruction, adynamic ileus, GI ischemia, or peritonitis.
A thorough surgical history is imperative prior to J-tube placement. Preexisting tubes, drains, mesh from previous hernia repairs, or stomas may require alternative planning. An extensive abdominal surgical history may prohibit safe laparoscopic J-tube placement and an open technique may be employed.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiologic workup is generally not necessary for J-tube placement. However, it is often the case that patients have had a plethora of upper abdominal imaging for other reasons that may provide valuable information or clues to previous unknown surgical procedures or unexpected anatomic findings.
SURGICAL MANAGEMENT
Preoperative Planning
The patient should be NPO for a minimum of 6 hours prior to the procedure.
Antibiotics should be given within 30 minutes of incision to reduce the incidence of abdominal wall infection around the tube site. First-generation cephalosporins are our preference when not contraindicated by the patient’s known allergies.
Generally, the jejunostomy feeding tube will exit the patient’s abdomen in the left upper quadrant (LUQ). As mentioned previously, preexisting tubes, drains, implanted mesh, and stomas may require tube site adjustment.
Positioning
For an open J-tube, the patient should be placed in the supine position. Usually, this procedure is done in addition to a larger procedure and thus the patient is already positioned accordingly.
For a laparoscopic J-tube, the patient should be positioned supine with the right arm tucked to allow for adequate room for the surgeon and assistant to both work comfortably on the right side.
It is important to be certain the patient is secured to the bed for intraoperative bed tilting, which may assist with exposure of the proximal jejunum.
TECHNIQUES
OPEN JEJUNOSTOMY TUBE PLACEMENT
Equipment
The type of tube used for the feeding jejunostomy is decided upon by the surgeon to optimize the longevity, comfort, and function for the patient. There are many commercially available tubes that vary widely in features, availability, and cost.
If a tube is being placed as part of a larger procedure and will likely be removed within 6 to 8 weeks, a standard 14-French (Fr) “red rubber Robinson” catheter is economical, time tested, and very functional.
The most important tube characteristics are that it should be soft, pliable, and preferentially not containing a balloon unless it is a small balloon, less than 5 mL, and specifically designed to be placed within the jejunum. Balloon catheters within the small bowel are a frequent cause of recurrent bowel obstructions and should be avoided.
The enteral end should be free of sharp edges that could damage the mucosa or promote migration or perforation. The holes should be of adequate size to allow feedings to pass through with minimal risk of clogging. The external portion should be tapered up to allow standard feeding pump tubing to be attached.
At our institution, a 12- to 18-Fr “red rubber Robinson” catheter is often used. Extra holes can be cut into the distal portion to allow tube feeds to flow with less resistance. These holes may be created by folding the tube over and cutting the corner of the fold (FIG 1). Alternatively, the tube from a laparoscopic jejunostomy kit can be used (Flexiflo Lap J™ laparoscopic jejunostomy kit by Abbott Nutrition).
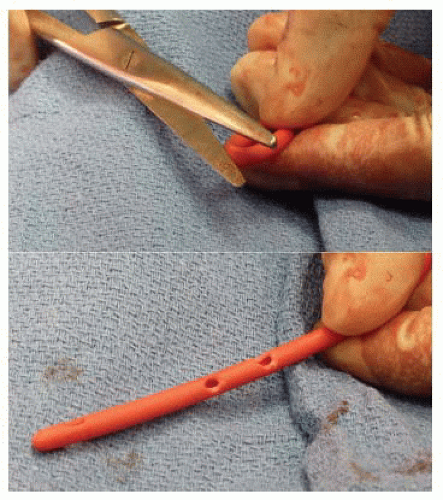 FIG 1 • Cutting extra holes in a red Robinson tube will reduce resistance of flow to the tube feeds. |
Incision
If the open J-tube placement is being done as a standalone operation, the incision should be centered in the midline at the level of the LOT.
The supraumbilical vertical midline incision should be carried through the linea alba with enough length to locate the LOT, mobilize 20 to 30 cm of jejunum, and allow for fixation of the jejunal segment to the peritoneum of the abdominal wall around the tube exit site. If there are minimal adhesions, this incision may be kept relatively small, 5 to 7 cm, and the majority of the operation can be done on eviscerated jejunum (FIG 2).
A limitation of an incision that is too small is that it may prove difficult to fix the bowel to the abdominal wall through the small incision. Exposure of this step should not be compromised in anyway to avoid lengthening the incision.
Mobilization of Jejunum
Once the peritoneal cavity has been entered, the omentum and transverse colon are retracted cephalad to expose the small bowel. A segment of small bowel is chosen in the LUQ and traced proximally until the LOT is identified.
Once the LOT is identified, the small bowel is examined all the way to the ileocecal valve to ensure no occult pathology, obstruction, or torsion is present.
The tube insertion site is chosen where the tube will pass through the abdominal wall. This will generally be in the LUQ. The surgeon must ensure the chosen segment of jejunum will reach the parietal surface of the abdominal wall without any tension or torsion. Lysis of adhesions may be needed to make sure the jejunum can reach the abdominal wall without tension.
Placement of atraumatic clamps on the left side of the fascia allows the abdominal wall to be retracted anteriorly for exposure of tube placement. While keeping retraction, a strong fine clamp is passed from inside the abdomen through the point chosen in the abdominal wall. A 3-mm skin incision, at the clamp exit site, is created and the tube is grasped and the distal end is pulled through the abdominal wall into the peritoneal cavity. Both ends of the tube are clamped together and positioned out of the way (FIG 3).
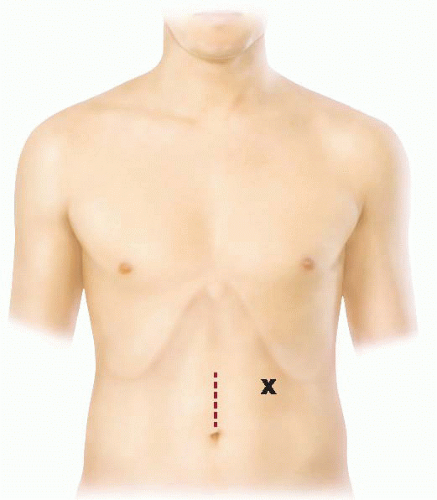 FIG 2 • Open incision diagram with tube exit site marked. |
Enterotomy and Placement of the Jejunostomy Tube
A segment of jejunum approximately 30 cm from the LOT is chosen as the site for the J-tube placement. This portion of jejunum can be eviscerated for the next steps if a smaller incision has been used. Using a 3-0 nonabsorbable or absorbable suture, place an approximately 4-mm purse-string suture in a box formation on the antimesenteric side of the small bowel (FIG 4). A double pursestring stitch may be used for additional security (FIG 5).
At this point, it is essential to note the proximal and distal ends of the jejunum and to ensure the orientation is maintained through the entire procedure.
Using cautery, create a small enterotomy in the center of the purse-string suture. It is helpful to grasp the bowel by the mesentery during this step. Inadvertent cautery injury to the opposite side of the small bowel can be avoided by cutting the serosa and muscularis with the cautery but “popping” into the lumen with a fine clamp (FIG 5).
Place the distal end of the feeding tube through the enterotomy into the lumen and direct it distally. The catheter is advanced until at least 10 cm is intraluminal. It can be advanced further if there is an excessive amount of tubing left externally (FIG 6).
Tie down the purse-string suture, taking care not to overtighten and occlude the tube (FIG 7).
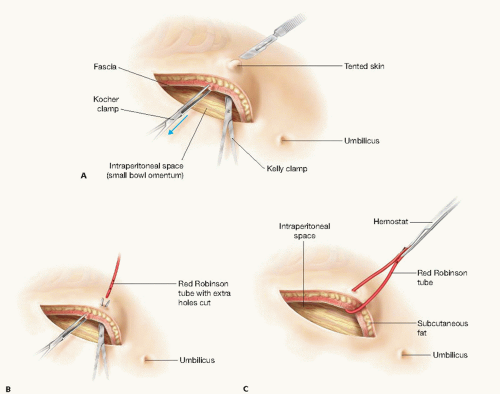
FIG 3 • Facial retraction anterior and midline with stab incision being made for the feeding tube.
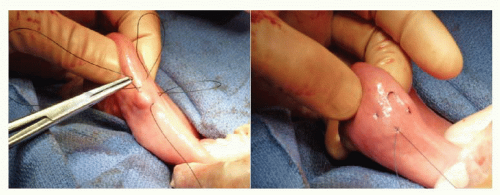
FIG 4 • Placement of purse-string stitch on antimesenteric jejunum.
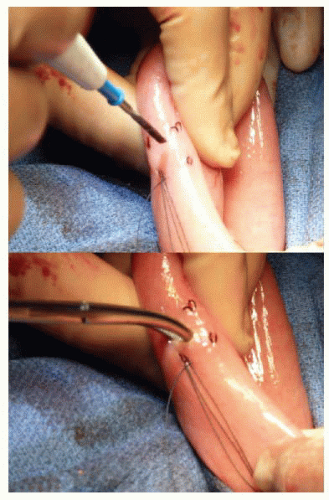
FIG 5 • The enterotomy is made with a cautery and then a hemostat is used to “pop” into the lumen. Note the double purse-string stitch used.
The tube entry sight is then imbricated using a threepoint triangular technique (FIG 8).
Next, a Witzel tunnel is created. Starting at the enterotomy, the small bowel is imbricated over the feeding tube using interrupted 3-0 absorbable suture on a taper needle (FIG 9) for a distance of about 5 cm. These are seromuscular bites spaced approximately 5 to 10 mm apart, ensuring the tube is not exposed. Care should be taken not to place the bites too far from the tube, as this will draw more bowel into the Witzel tunnel and narrow the jejunal lumen (FIG 10).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


