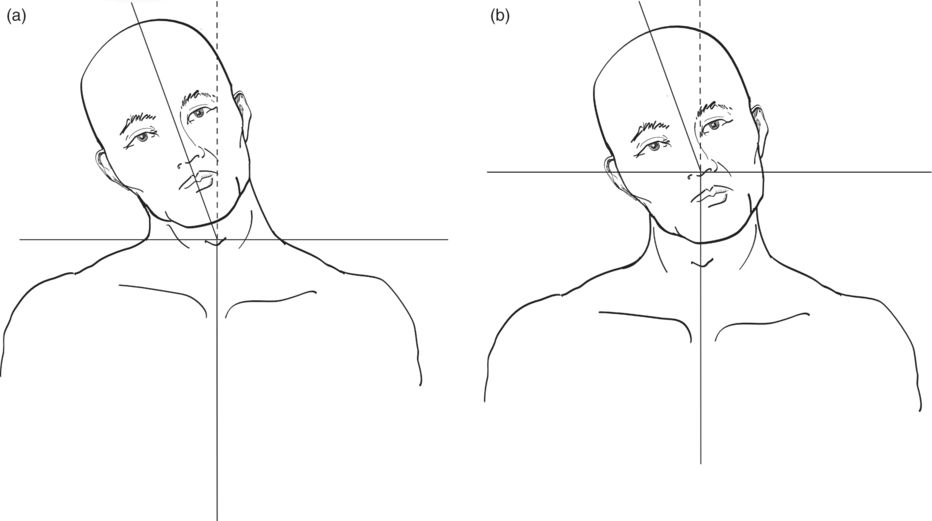
Fig. 6.1 Lateral shift or forward sagittal shift. (a) Lateral shift to the right: laterocollis to the right. The head is tilted on the neck line to the left: laterocaput to the left. (b) Sagittal shift forward: antecollis. The head is tilted in the neck line backward: retrocaput.
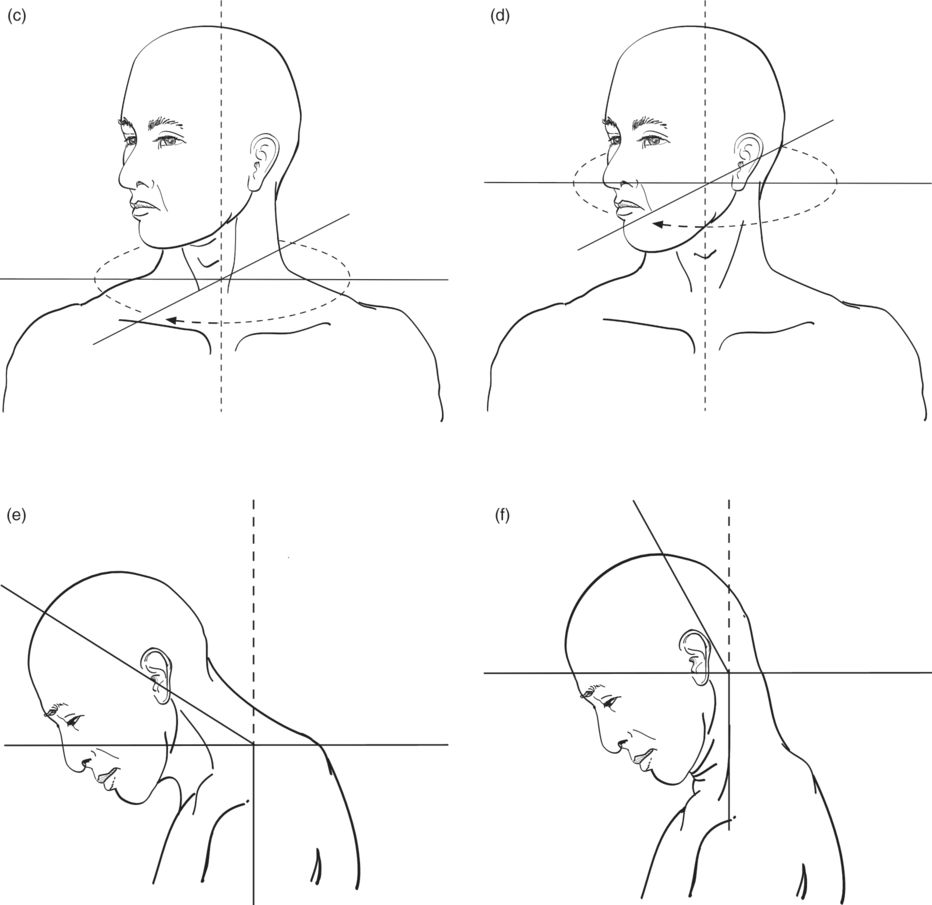
The more differentiated is the examination of the patient, the better the likely success of therapy. Cervical dystonia may occur in principle in three axes (rotation, lateral flexion and sagittal flexion). The head or the neck can be affected alone in each of these planes of movement. Therefore, eight clinical forms can be distinguished: torticollis, laterocollis, antecollis, retrocollis, torticaput, laterocaput, antecaput and retrocaput (Fig. 6.2). In each plane of motion, the variations in the ratio 1:1:3 for each condition, such as for head turning, would be 1 torticollis pure to 1 pure torticaput to 3 both variants (Reichel, 2012).
Fig. 6.2 The eight basic forms of cervical dystonia: (a) laterocollis; (b) laterocaput; (c) torticollis; (d) torticaput; (e) antecollis; (f) antecaput; (g) retrocollis; (h) retrocaput.
Moreover, almost all types can occur at different levels together in combination: most common are the combination of lateral tilting and rotation.
Clinical studies and additional examinations
Observation of the patient in a sitting position from the front
The patient should assume a relaxed position on a swivel chair. The patient is asked to lean the upper body to the back of the chair with the eyes closed. The face is turned toward the examiner. The position of the head is observed in relaxation. The patient is asked to conduct the following movements:
- rotation of the head to the left and right and take a subjective center position
- tilting of the head to the left and right and then taking a subjective center position.
Observation of the patient in a sitting position from the side
The patient is again asked to take the relaxed sitting position and rotate so that he or she can be seen from the side. Throughout the investigation, the patient leans the upper body against the back of the chair and has eyes closed. The head position is observed in relaxation. Upon request, the patient moves through the following motions:
- tilting the head forward then returning to a subjective neutral head position
- tilting the head backward then returning to a subjective neutral head position.
Investigation of the rotation: torticollis and torticaput
To distinguish between a torticollis and torticaput (Fig. 6.3), one must differentiate whether the area the rotation is in the range C3–C7 (torticollis), or in the lower head joint between C1 and C2 (torticaput). A mark (skin marker) is placed at the larynx above the superior thyroid notch and above the jugular notch at the manubrium sterni. If the mark on the throat shifts laterally from the mark on the manubrium at the turn of the head, this indicates the presentation of torticollis (Fig. 6.4a). In torticaput, the two marks stay perpendicular to each other on head rotation (Fig. 6.4b).
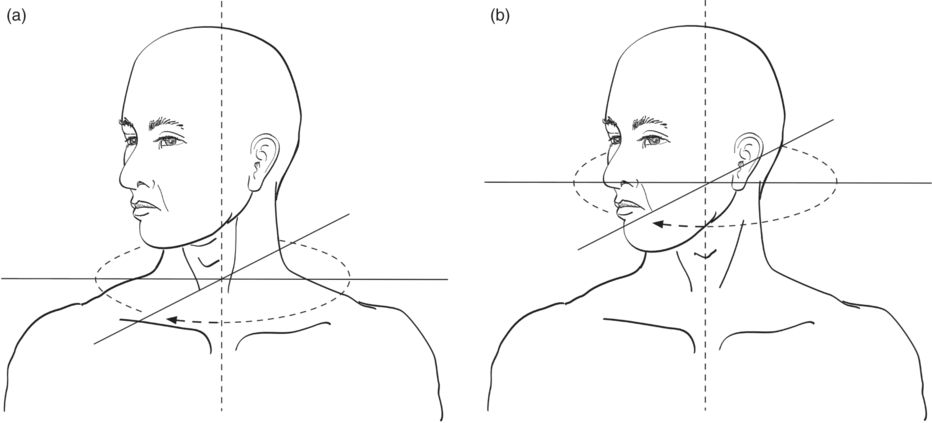
Fig. 6.3 Scheme of dystonic head rotation. (a) Rotation below C2 is torticollis. (b) Rotation in the lower head joint (between C1 and C2) is torticaput.

Fig. 6.4 Patients with head rotation. (a) The thyroid notch is clearly on the side of the jugular notch in torticollis. (b) The thyroid notch is located vertically above the jugular notch in torticaput.
When the analysis is uncertain, CT of the neck may help to clarify the situation, with a CT slice at the C3 level. The relationship between the position of C3 and the chin may help to clarify torticollis from torticaput.
In torticollis, C3 and the chin align in one direction, which indicates the rotation occurs below C3 (Fig. 6.5a). In torticaput, there is a rotation of the chin against C3, which indicates that the rotation occurs above C3, that is, at the lower head joint (Fig. 6.5b). For this differentiation, pictures from the CT bone window may be adequate.
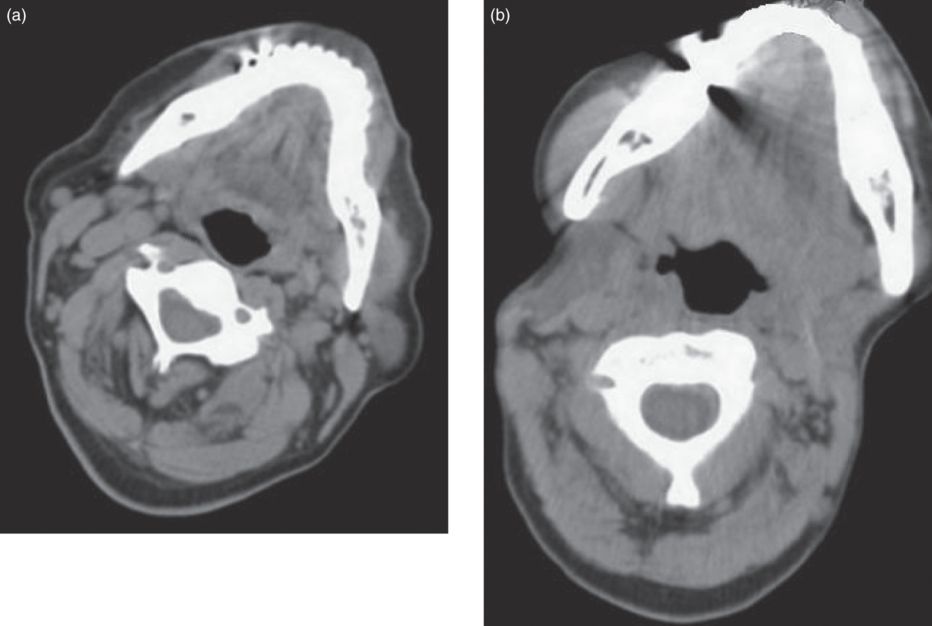
Fig. 6.5 The neck at the level of C3 in CT scans. (a) In torticollis, C3 and the chin point in one direction; (b) in torticaput, the chin is rotated compared with C3.
In torticaput, the obliquus capitis inferior is often involved (Reichel, 2011). On CT, a short thick muscle on the side of the rotation at the level of the lower head–spine junction can be seen, with an elongated thinner muscle on the opposite side (Fig. 6.6a). In the CT reconstruction, the asymmetry of the obliquus capitis inferior muscles on either side can be seen in the coronal section (Fig. 6.6b).
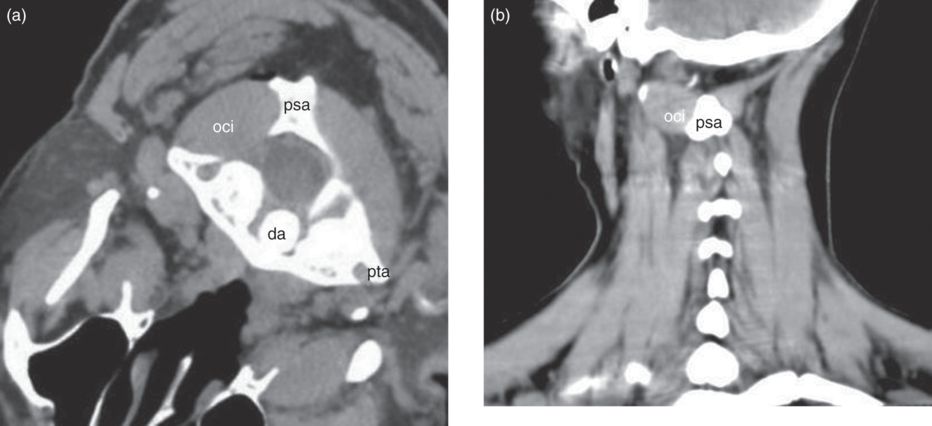
Fig. 6.6 The obliquus capitis inferior muscle. (a) The patient lies on her stomach for this view. In axial section, the dystonic obliquus capitis inferior (oci) is shown as thick and shortened. Note that the normal obliquus capitis inferior muscle of the opposite side is long and slender. (b) In the reconstruction (coronal section), the asymmetry of the obliquus capitis inferior muscle is evident. da, dens of the axis; psa, spinal process of the axis; pta, transverse process of the atlas.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


