Usually represents liver involvement by infectious mononucleosis
Elevated serum transaminase, alkaline phosphatase, and bilirubin levels
Self limited in majority of cases
• EBV-associated lymphoproliferative disorders
In immunocompromised individuals due to uncontrolled EBV replication
Occurs in 1.0-2.8% of liver transplants
• Asymptomatic lifelong infection in > 90% of world adult population
Microscopic
• EBV hepatitis
Diffuse sinusoidal lymphocytic infiltration in Indian file or string of beads pattern
Mixed inflammatory cell infiltrates in portal tracts, consisting predominantly of lymphocytes
Scattered large and irregular (atypical) lymphocytes in sinusoids and portal tracts
• Hepatic PTLD
Morphology ranges from hepatitis-like to lymphoma
Ancillary Tests
• Detection of EBV early RNA (EBER) on tissue sections by in situ hybridization
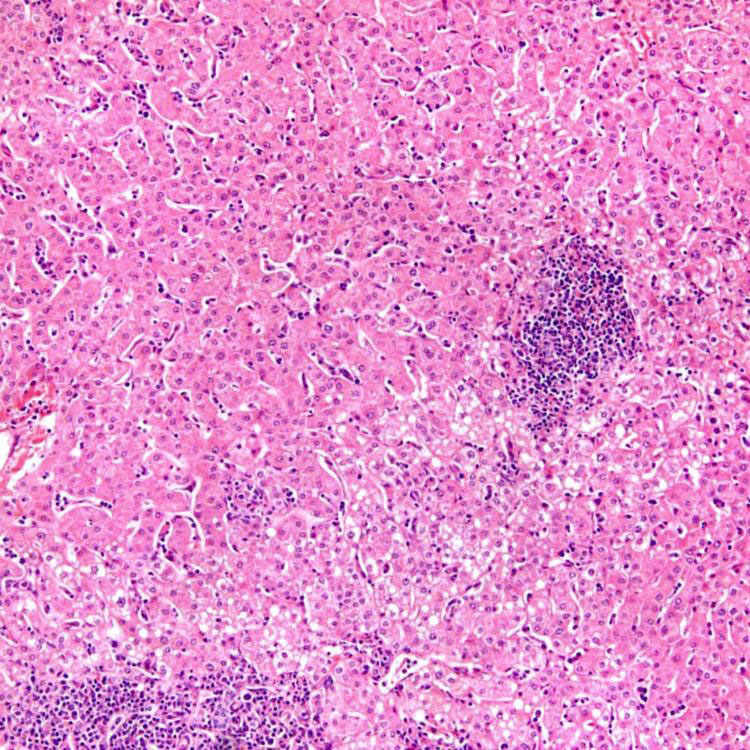
Portal and Lobular Inflammation Epstein-Barr virus (EBV) hepatitis is characterized by portal and lobular inflammation consisting predominantly of lymphocytes. Prominent sinusoidal lymphocytes can be appreciated even at this low power. There is also mild steatosis, unrelated to EBV infection.
Portal and Sinusoidal Lymphocytosis This case of EBV hepatitis shows portal and lobular lymphocytic infiltrates. Note the string of beads linear pattern of lymphocytes in the sinusoids.
String of Beads Sinusoidal Infiltrates A characteristic finding of EBV hepatitis is a diffuse sinusoidal lymphocytic infiltrate with an Indian file or string of beads pattern . Occasional atypical lymphocytes are noted. Hemophagocytosis, which can be seen in EBV hepatitis, is not observed in this case.
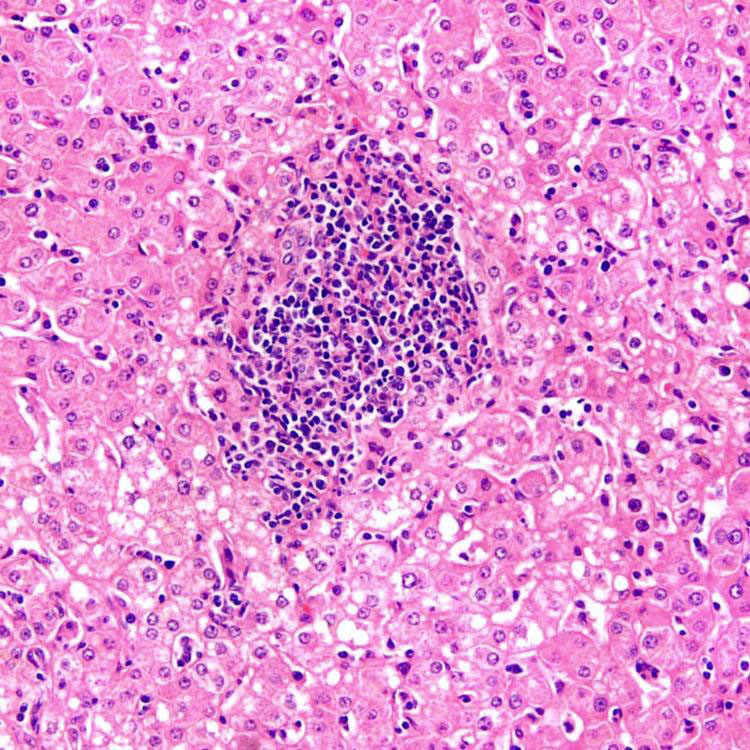
Portal Inflammation Occasionally, EBV hepatitis features a florid portal infiltrate consisting of lymphocytes (some of which may be atypical) and histiocytes. Note the surrounding sinusoidal lymphocytosis.
TERMINOLOGY
Abbreviations
• Epstein-Barr virus (EBV)
Definitions
• Infection by EBV
In liver, may cause either hepatitis or posttransplant lymphoproliferative disorder (PTLD)
ETIOLOGY/PATHOGENESIS
Infectious Agents
• Member of herpesvirus family (human herpesvirus-4)
Double-stranded DNA virus
• Transmission via intimate contact, frequently with saliva of infected person
Infection begins in oropharyngeal lymphoid tissues, particularly tonsils
Viral envelop glycoprotein binds to CD21 (CR2) on B lymphocytes
CLINICAL ISSUES
Epidemiology
• New infection typically occurs during adolescence or young adulthood in developed countries
Infectious mononucleosis 35-50% of time
• Typically occurs in 1st few years of life in developing countries with universal seroconversion by 3-4 years of age
Usually asymptomatic
• Asymptomatic lifelong infection in > 90% of world adult population








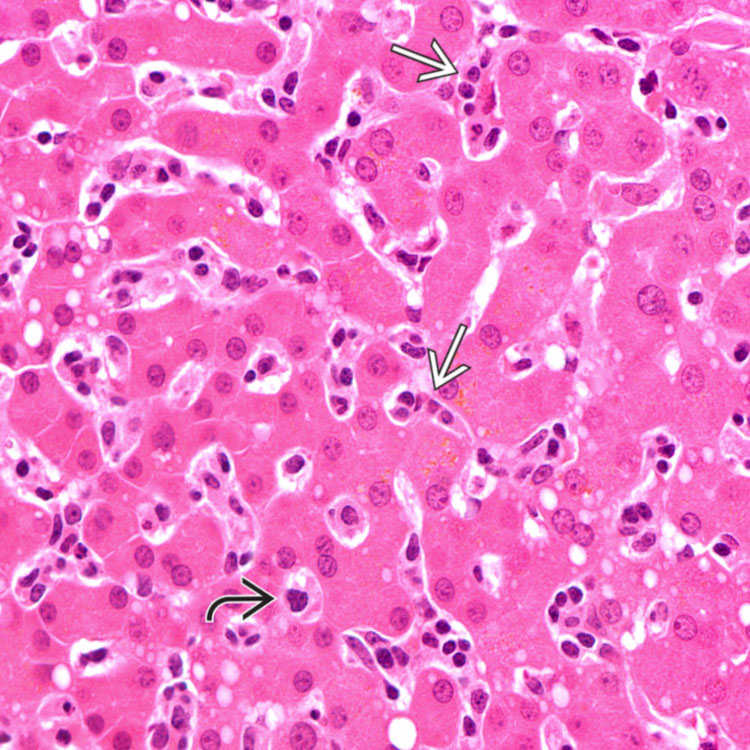
 . Occasional atypical lymphocytes
. Occasional atypical lymphocytes  are noted. Hemophagocytosis, which can be seen in EBV hepatitis, is not observed in this case.
are noted. Hemophagocytosis, which can be seen in EBV hepatitis, is not observed in this case.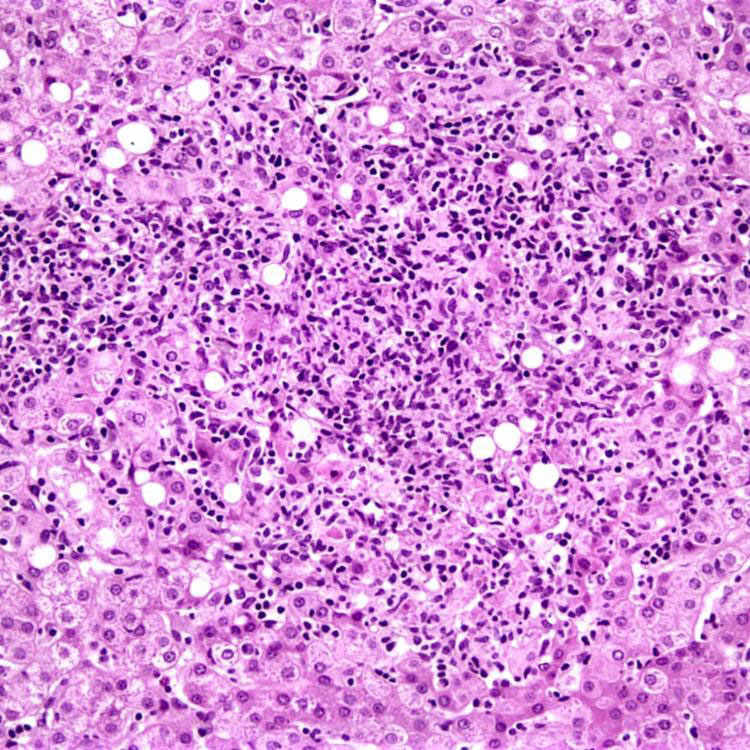








 Fever, fatigue, malaise, sore throat, arthralgia, jaundice, lymphadenopathy, splenomegaly, and hepatomegaly
Fever, fatigue, malaise, sore throat, arthralgia, jaundice, lymphadenopathy, splenomegaly, and hepatomegaly












