Multicentricity at presentation likely represents locoregional metastases
• Treatment: Wide surgical excision with negative margins
• Indolent clinical course in majority of cases
• Metastases in 20-30%
• Overall mortality rate of 10-20%
High-risk EHE features size > 3 cm and > 3 mitoses/50 HPF
– Associated with significant decrease in survival
Microscopic
• Infiltrative growth with absence of defined lobularity
• Epithelioid eosinophilic cells arranged in cords, nests
Intracytoplasmic vacuoles common (blister cells)
• Well-formed vascular channels typically absent
• Characteristic myxoid to hyaline stromal matrix
• Involvement of larger vessels common
Ancillary Tests
• CD31(+), CD34(+), ERG(+), FLI-1(+)
• Nuclear TFE3(+) observed in distinctive genetic subset
• Keratin (+) in up to 35% of cases, often focal
• Molecular: t(1;3)(p36;q25) with WWTR1 – CAMTA1
Distinctive subset contains YAP1 – TFE3 fusion
Top Differential Diagnoses
• Epithelioid hemangioma
• Epithelioid angiosarcoma
• Epithelioid sarcoma
• Myoepithelioma of soft tissue
Epithelioid Hemangioendothelioma: Clinical Photo Clinical photograph shows a rare cutaneous epithelioid hemangioendothelioma (EHE) presenting as an exophytic lesion.
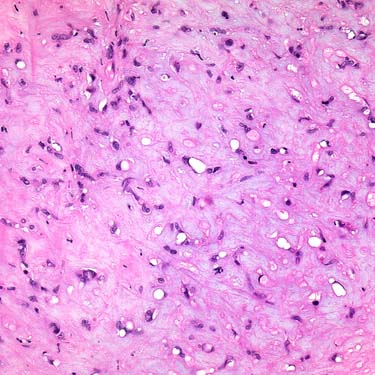
Epithelioid Hemangioendothelioma EHE is a distinctive malignant vascular neoplasm characterized predominantly by cords of epithelioid tumor cells within a characteristic myxoid to hyaline matrix.
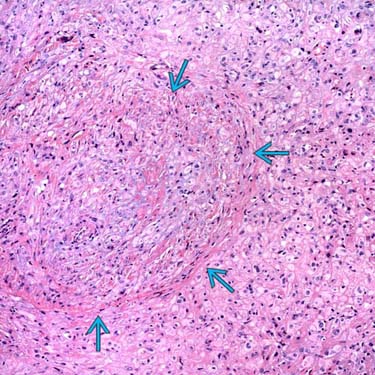
EHE With Involvement of Larger Vessel EHE is an angiocentric neoplasm and evidence of origin from a larger vessel may be evident histologically. Note the residual smooth muscle wall in this image. Tumor cells often extend outward from the involved vessel into the surrounding tissues.
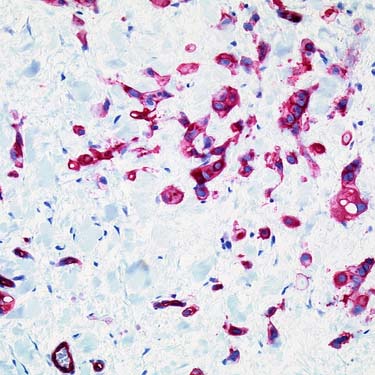
CD31 Expression by Immunohistochemistry EHE shows expression of endothelial markers, including CD31 (shown), CD34, ERG, and FLI-1. Focal keratin positivity is seen in up to 1/3 of cases.
TERMINOLOGY
Abbreviations
• Epithelioid hemangioendothelioma (EHE)
Synonyms
• Intravascular bronchioloalveolar tumor (lung)
Definitions
• Malignant angiocentric vascular neoplasm composed of epithelioid endothelial cells within characteristic myxohyaline stromal matrix
CLINICAL ISSUES
Epidemiology
• Incidence
Rare tumors
• Age
Wide age range affected
– Most common in 30- to 50-year-old patients
– Rare in childhood
• Sex
Slight female predominance
Site
• Wide distribution in soft tissue
Extremities, head/neck region, others
• Visceral organs (particularly liver and lung)
Presentation
• Solitary, often painful mass
Superficial or deep
Rarely cutaneous
• Apparent multicentricity at time of presentation (up to 50% of cases)
Recent molecular data supports conclusion of locoregional metastases over multiple primary lesions
• Occlusion of vessels
30-50% of cases arise in or are associated with preexisting vessel
May cause more profound vasoocclusive symptoms, including edema
Treatment
• Wide surgical excision with negative margins
• No proven role for adjuvant chemotherapy &/or radiotherapy
Prognosis
• Indolent clinical course in majority of cases
Local recurrence in 10-15%
• Metastases in 20-30%
Usually to liver, bone, lungs
Occasionally regional lymph nodes
• Overall mortality rate of 10-20%
• Proposed risk assessment
High-risk EHE features size > 3 cm and > 3 mitoses per 50 HPF
– Significant decrease in survival in these cases
MACROSCOPIC
General Features
• Well-circumscribed nodular lesion
• Firm, tan-gray cut surface
• Intravascular tumors may simulate organizing thrombi
Size
• Wide size range
Mean: 2.5 cm in 1 large series
MICROSCOPIC
Histologic Features
• Infiltrative growth with absence of defined lobularity
• Epithelioid cells arranged in cords, singly, and in small aggregates or nests




 in this image. Tumor cells often extend outward from the involved vessel into the surrounding tissues.
in this image. Tumor cells often extend outward from the involved vessel into the surrounding tissues.