Overview
The list of toxins the human body can be exposed to is extensive. Since the list of toxins and their pathologic effects is so numerous, only some of the major toxins and their effects will be discussed in this chapter. Of these, by far the two most commonly encountered toxins are tobacco smoke and alcohol. In addition to a few major toxins, this chapter will also discuss very basic physical trauma and nutritional deficiencies.
The metabolism of xenobiotics (i.e., mechanism for removal of foreign substances such as drugs from the body) occurs via two phases. Phase I reactions involve attachment of polar functional groups to the substance, and phase II reactions involve conjugation of the substance. One important point concerning therapeutic implications is the concept that genetic variations in levels of cytochrome P-450 isozymes produce both “rapid metabolizers” and “slow metabolizers” and can result in toxic levels of medication in a patient on an otherwise normal therapeutic dose.
Some Selected Toxic Substances
Constituents: Polycyclic aromatic hydrocarbons, arsenic, nickel, carbon monoxide, hydrogen cyanide, nicotine.
Effects of nicotine: Increased heart rate, increased blood pressure.
Important points
- About 30% of all cancer deaths and 90% of all lung cancer deaths are related to smoking.
- Pregnant females who smoke 10 or more cigarettes a day can induce hypoxia in their fetuses, which leads to complications that include decreased fetal weight and prematurity and to premature rupture of membranes and placental abruption at the time of delivery.
Toxic levels
- Naïve users: 0.3 to 0.4 mg/dL can result in coma or death.
- Tolerant users: Can develop levels up to 0.7 mg/dL.
Complications of ethanol use by organ system
- Liver: Fatty change; hepatitis due to direct toxic effect of ethanol on hepatocytes; and cirrhosis, which occurs in only 10–15% of chronic alcoholics.
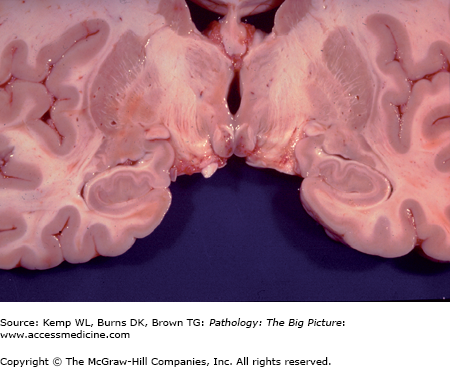
- Central nervous system (CNS): Thiamine deficiency, which may present as Wernicke encephalopathy (Figure 5-1) or Korsakoff syndrome (amnesia and confabulation). Morphologic features of thiamine deficiency include periventricular hemorrhage and petechiae of the mammillary bodies and cerebellar atrophy. Complications of ethanol use include alcohol withdrawal and associated delirium tremens.
- Cardiovascular: Dilated cardiomyopathy, hypertension.
- Gastrointestinal: Gastritis, pancreatitis.
- Reproductive: Fetal alcohol syndrome is associated with mental retardation, microcephaly, maxillary hypoplasia, smooth philtrum, short palpebral fissure, and atrial septal defects.
Mechanism: Chronic alcohol use causes depression of α-receptors and β-receptors and enhances γ-aminobutyric acid (GABA), which serve as a stimulus to increase baseline neuronal activity. Therefore, when alcohol is withdrawn, patients have a sudden excited state of CNS activity because the depressive effect of the alcohol is removed.
Clinical presentation: Tachycardia, hypertension, tremulousness, and hyperreflexia.
Complications of alcohol withdrawal: Seizures (10%); hallucinations, usually visual (25%); and delirium tremens (5%). Severe alcohol withdrawal is life threatening, causing dehydration, hyperthermia, and electrolyte imbalances. A cardiac dysrhythmia can occur due to hypokalemia or hypomagnesemia.
- Delirium tremens: Confusion, disorientation, tactile hallucinations (often of bugs on skin), and marked tremor.
Treatment of alcohol withdrawal: Benzodiazepines; treatment of dehydration and electrolyte disturbances.
Mechanism
- Blocks reuptake of dopamine, activating reward centers in the CNS.
- Blocks reuptake of norepinephrine and epinephrine, leading to vascular constriction.
Complications: Sudden cardiac death, atherosclerosis, cardiac hypertrophy, intracerebral hemorrhage, rhabdomyolysis, placental abruption.
Source
- Occupational: Painting, foundry work, mining.
- Nonoccupational: Children eating lead-based paint chips.
Complications: Anemia; chronic renal tubulointerstitial disease; in children, bone defects.
Clinical presentation: In children, abdominal pain is a common complaint. Findings include microcytic hypochromic anemia with basophilic stippling of red blood cells and lead lines on the gingivae and in long bones seen on plain films. Encephalopathy is seen in severe cases. Saturnine gout is characterized by the triad of lead nephropathy, gout, and hypertension, and is associated with homemade “moonshine” produced in lead-containing stills.
Mechanism: Colorless gas with the odor of almonds. It binds and inactivates cytochromes of the electron transport chain, thus inhibiting the biochemical pathway of respiration.
Clinical presentation: Commonly seen with smoke inhalation; occasionally seen with nitroprusside toxicity. Patients have rapid onset of weakness, shortness of breath, convulsions, and coma. Patients present with cherry red skin due to impaired extraction of oxygen from hemoglobin.
Mechanism: Hemoglobin has 200 times more affinity for carbon monoxide than for oxygen. Carboxyhemoglobin binds oxygen more avidly, resulting in impaired delivery of oxygen to tissues.
Presentation: Common in smoke inhalation, enclosed exposure to automobile exhaust, or in the wintertime with home furnaces. Patients present with cherry red skin (classic), flu-like symptoms, headache, and neurologic symptoms (Figure 5-2).
Figure 5-2.

Cherry-red lividity due to carbon monoxide poisoning. This man committed suicide by remaining in a car with the windows closed and the engine running. Carbon monoxide produces a bright red discoloration of the blood. In this case, the lividity (postmortem change due to settling of the blood in dependent regions of the body) is cherry red in color instead of the usual red-purple, due to the carbon monoxide, which is irreversibly bound to the hemoglobin.
Acute disease: Features include atrophy of bone marrow, erythema of skin, edema and ulcers of the gastrointestinal tract, and edema and necrosis of the brain.



