Endocervical Glandular Hyperplasia (Diffuse and Lobular)
Marisa R. Nucci, MD
Key Facts
Clinical Issues
Typically incidental finding
Excellent prognosis
If atypical features present in LEGH, may be associated with adenoma malignum
Microscopic Pathology
Diffuse laminar endocervical glandular hyperplasia
Usually inner 1/3 of cervical wall
Laminar proliferation of round to branching glands
Mild nuclear enlargement with nucleoli (reactive changes) associated with stromal chronic inflammation, the latter more pronounced at deepest interface
Lobular endocervical glandular hyperplasia
Usually inner half of cervical wall
Lobular proliferation of small to medium-sized rounded glands often centered around larger gland
Tall columnar mucinous epithelium with bland, basally located nuclei
LEGH with atypical features
Epithelial infolding or distinct papillary projections
Loss of nuclear polarity with budding or “exfoliation”
Nuclear enlargement with hyperchromasia and distinct nucleoli
Apoptotic bodies &/or luminal debris
Occasional apical mitoses
Top Differential Diagnoses
Minimal deviation adenocarcinoma (adenoma malignum)
Endocervical adenomyoma
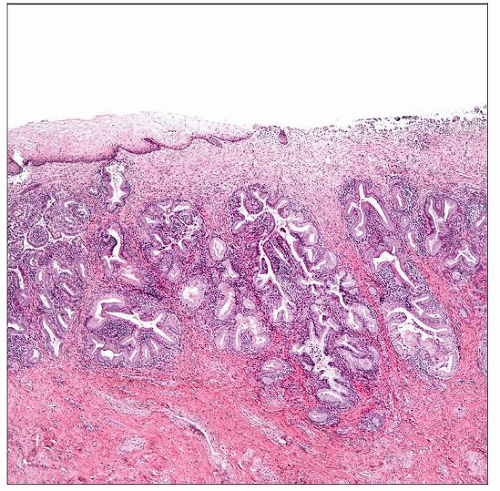 Diffuse laminar endocervical glandular hyperplasia shows a band-like proliferation of irregularly shaped glands that have a sharply demarcated deep border. Note the associated inflammatory infiltrate. |
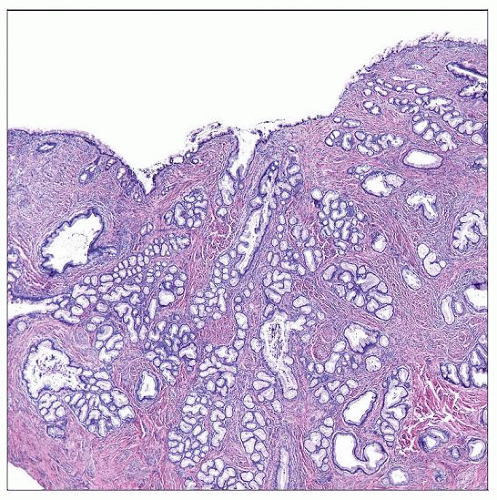 Lobular endocervical glandular hyperplasia is characterized by a lobular proliferation of small to medium-sized round glands often centered around a larger gland with a clefted contour. |
TERMINOLOGY
Abbreviations
Diffuse endocervical glandular hyperplasia (DEGH)
Lobular endocervical glandular hyperplasia (LEGH)
Definitions
Benign proliferation of endocervical glands
CLINICAL ISSUES
Presentation
Typically incidental finding
Vaginal (sometimes mucoid) discharge (LEGH)
Treatment
If atypical features present, complete excision to exclude coexistent malignancy
Prognosis
Excellent (DEGH, LEGH)
LEGH with atypical architectural or cytologic features may be associated with adenoma malignum, the latter associated with poor prognosis
MACROSCOPIC FEATURES
Diffuse Laminar Endocervical Glandular Hyperplasia
Typically no appreciable mass
Lobular Endocervical Glandular Hyperplasia
Often no gross lesion
Occasionally grossly visible, well-demarcated mass
MICROSCOPIC PATHOLOGY
Histologic Features
Diffuse laminar endocervical glandular hyperplasia
Usually inner 1/3 of cervical wall
Sharply demarcated deep border
Laminar proliferation of round to branching glands
Chronic inflammatory infiltrate, more pronounced at deepest interface
Lobular endocervical glandular hyperplasia
Usually inner half of cervical wall
Lobular proliferation of small to medium-sized rounded glands often centered around larger gland
No associated stromal response
LEGH with atypical features
Epithelial infolding or distinct papillary projections
Budding or “exfoliation” of cells
Cytologic Features
Diffuse laminar endocervical glandular hyperplasia
Tall columnar mucinous epithelium
Mild nuclear enlargement with nucleoli (reactive changes) associated with stromal inflammation
Lobular endocervical glandular hyperplasia
Tall columnar mucinous epithelium
Cytoplasm may have eosinophilic, granular appearance (gastric-type differentiation)
Bland, basally located nuclei
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


