High-Yield Terms to Learn
Lipoproteins Macromolecular complexes in the blood that transport lipids Apolipoproteins Proteins on the surface of lipoproteins; they play critical roles in the regulation of lipoprotein metabolism and uptake into cells Low-density lipoprotein (LDL) Cholesterol-rich lipoprotein whose regulated uptake by hepatocytes and other cells requires functional LDL receptors; an elevated LDL concentration is associated with atherosclerosis High-density lipoprotein (HDL) Cholesterol-rich lipoprotein that transports cholesterol from the tissues to the liver; a low concentration is associated with atherosclerosis Very-low-density lipoprotein (VLDL) Triglyceride- and cholesterol-rich lipoprotein secreted by the liver that transports triglycerides to the periphery; precursor of LDL HMG-CoA reductase 3-Hydroxy-3-methylglutaryl-coenzyme A reductase; the enzyme that catalyzes the rate-limiting step in cholesterol biosynthesis Lipoprotein lipase (LPL) An enzyme found primarily on the surface of endothelial cells that releases free fatty acids from triglycerides in lipoproteins; the free fatty acids are taken up into cells Proliferator-activated receptor-alpha (PPAR- ) Member of a family of nuclear transcription regulators that participate in the regulation of metabolic processes; target of the fibrate drugs
) Member of a family of nuclear transcription regulators that participate in the regulation of metabolic processes; target of the fibrate drugs
Hyperlipoproteinemia
Pathogenesis
Premature or accelerated development of atherosclerosis is strongly associated with elevated concentrations of certain plasma lipoproteins, especially the low-density lipoproteins (LDL) that participate in cholesterol transport. A depressed level of high-density lipoproteins (HDL) is also associated with increased risk of atherosclerosis. In some families, hypertriglyceridemia is similarly correlated with atherosclerosis. Chylomicronemia, the occurrence of chylomicrons in the serum while fasting, is a recessive trait that is correlated with a high incidence of acute pancreatitis and managed by restriction of total fat intake (Table 35-1).
TABLE 35-1 Primary hyperlipoproteinemias and their drug treatment.
Condition/Cause Manifestations, Cause Single Drug Drug Combination Primary chylomicronemia Chylomicrons, VLDL increased; deficiency in LPL or apoC-II Niacin, fibrate Niacin plus fibrate Familial hypertriglyceridemia Severe VLDL, chylomicrons increased; decreased clearance of VLDL Niacin, fibrate Niacin plus fibrate Moderate VLDL increased, chylomicrons may be increased; increased production of VLDL Niacin, fibrate Familial combined hyperlipoproteinemia Increased hepatic apoB and VLDL production VLDL increased Niacin, fibrate, statin Two or 3 of the individual drugs LDL increased Niacin, statin, ezetimibe Two or 3 of the individual drugs VLDL, LDL increased Niacin, statin Niacin or fibrate plus statin Familial dysbetalipoproteinemia VLDL remnants, chylomicron remnants increased; deficiency in apoE Fibrate, niacin Fibrate plus niacin, or either plus statin Familial hypercholesterolemia LDL increased; defect in LDL receptors Heterozygous Statin, resin, niacin, ezetimibe Two or 3 of the individual drugs Homozygous Niacin, atorvastatin, rosuvastatin, ezetimibe Niacin plus statin plus ezetimibe
Modified and reproduced, with permission, from Katzung BG, editor: Basic & Clinical Pharmacology, 11th ed. McGraw-Hill, 2009.
Regulation of plasma lipoprotein levels involves a complex interplay of dietary fat intake, hepatic processing, and utilization in peripheral tissues (Figure 35-1). Primary disturbances in regulation occur in a number of genetic conditions involving mutations in apolipoproteins, their receptors, transport mechanisms, and lipid-metabolizing enzymes. Secondary disturbances are associated with a Western diet, many endocrine conditions, and diseases of the liver or kidneys.
FIGURE 35-1
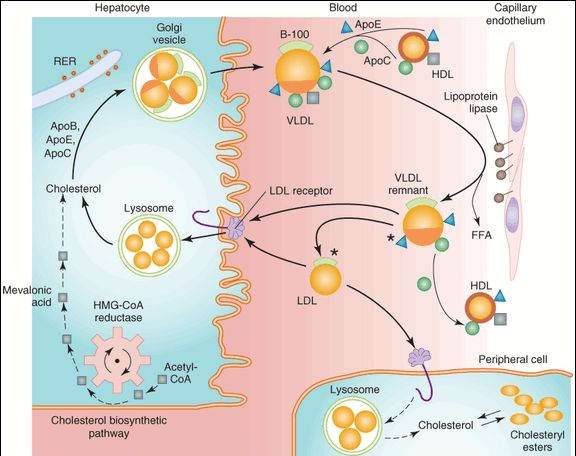
Metabolism of lipoproteins of hepatic origin. The heavy arrows show the primary pathways. Nascent VLDL are secreted via the Golgi apparatus. They acquire additional apoC lipoproteins and apoE from HDL. VLDL is converted to VLDL remnants by lipolysis via lipoprotein lipase associated with capillaries in peripheral tissue supplies. In the process, C apolipoproteins and a portion of apoE are given back to HDL. Some of the VLDL remnants are converted to LDL by further loss of triglycerides and loss of apoE. A major pathway for LDL degradation involves the endocytosis of LDL by LDL receptors in the liver and the peripheral tissues, for which apoB-100 is the ligand. Dark color denotes cholesteryl esters; light color, triglycerides; the asterisk denotes a functional ligand for LDL receptors; triangles indicate apoE; circles and squares represent C apolipoproteins. FFA, free fatty acid; RER, rough endoplasmic reticulum.
(Reproduced, with permission, from Katzung BG, editor: Basic & Clinical Pharmacology, 11th ed. McGraw-Hill, 2009: Fig. 35-1.)
Treatment Strategies
Diet
Cholesterol and saturated fats are the primary dietary factors that contribute to elevated levels of plasma lipoproteins. Dietary measures designed to reduce the total intake of these substances constitute the first method of management and may be sufficient to reduce lipoprotein levels to a safe range. Because alcohol raises triglyceride and very-low-density lipoprotein (VLDL) levels, it should be avoided by patients with hypertriglyceridemia.
Drugs
For an individual patient, the choice of drug treatment is based on the lipid abnormality. The drugs that are most effective at lowering LDL cholesterol include the HMG-CoA reductase inhibitors, resins, ezetimibe, and niacin. The fibric acid derivatives (eg, gemfibrozil) and niacin are most effective at lowering triglyceride and VLDL concentrations and raising HDL cholesterol concentrations (Table 35-2).
TABLE 35-2 Lipid-modifying effects of antihyperlipidemic drugs.
Drug or Drug Group LDL Cholesterol HDL Cholesterol Triglycerides Statins Atorvastatin, rosuvastatin, simvastatin -25 to -50% +5 to +15% 
 Lovastatin, pravastatin -25 to -40% +5 to +10%
Lovastatin, pravastatin -25 to -40% +5 to +10%  Fluvastatin -20 to -30% +5 to +10%
Fluvastatin -20 to -30% +5 to +10%  Resins -15 to -25% +5 to +10% ±a
Resins -15 to -25% +5 to +10% ±a
Ezetimibe -20% +5% ± Niacin -15 to -25% +25 to +35% 
 Gemfibrozil -10 to -15%b
Gemfibrozil -10 to -15%b
+15 to + 20% 

LDL, low-density lipoprotein; HDL, high-density lipoprotein; ±, variable, if any.
aResins can increase triglycerides in some patients with combined hyperlipidemia.
bGemfibrozil and other fibrates can increase LDL cholesterol in patients with combined hyperlipidemia.
Modified and reproduced, with permission, from McPhee SJ, Papadakis MA, Tierney LM, editors: Current Medical Diagnosis & Treatment, 46th ed. McGraw-Hill, 2006.
HMG-CoA Reductase Inhibitors
Mechanism and Effects
The rate-limiting step in hepatic cholesterol synthesis is conversion of hydroxymethylglutaryl coenzyme A ( HMG-CoA) to mevalonate by HMG-CoA reductase. The statins
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


