• Symptoms may present after months to years of therapy
Patients may be asymptomatic despite liver injury
• Due to long half-life of amiodarone, may take months to see improvement
• Risk of liver damage with methotrexate use depends on duration of therapy and dose
Exacerbated by concomitant obesity, alcohol use
• Patients with drug-induced phospholipidosis often also have history of alcohol use or risk factors for nonalcoholic steatohepatitis, confounding clinical picture
Microscopic
• Amiodarone
Steatosis
Phospholipidosis
Mallory hyaline, often with associated neutrophils (satellitosis)
• Methotrexate
Steatosis
Reactive changes
Fibrosis
Grading scheme exists for purposes of clinical decision making
– Grades I-IV; drug usually stopped at IIIB-IV
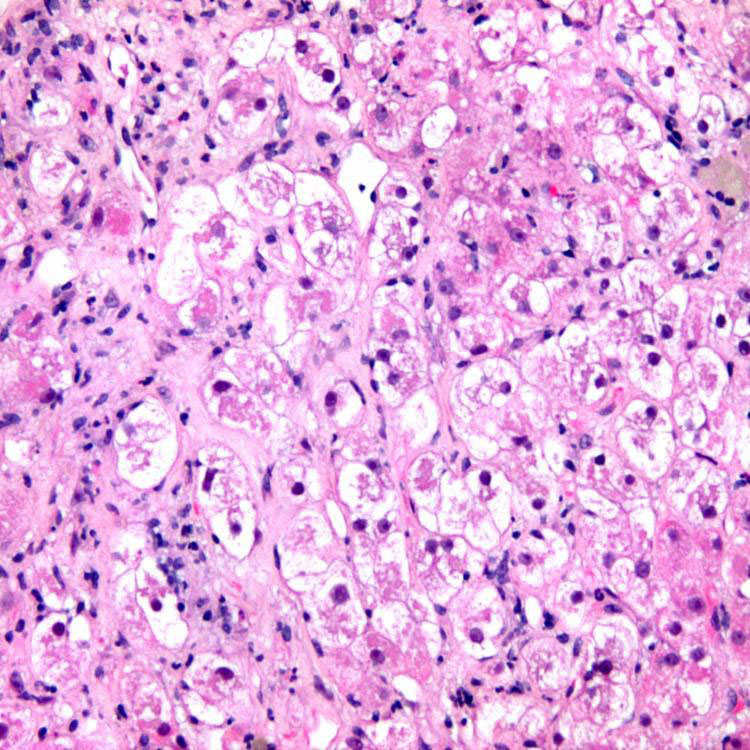
Amiodarone, Ballooned Hepatocytes Amiodarone toxicity typically features ballooned hepatocytes with abundant Mallory hyaline.
Amiodarone, Mallory Hyaline and Satellitosis of Neutrophils Features of amiodarone hepatotoxicity include foamy, ballooned hepatocytes and abundant Mallory hyaline with surrounding neutrophils (satellitosis).
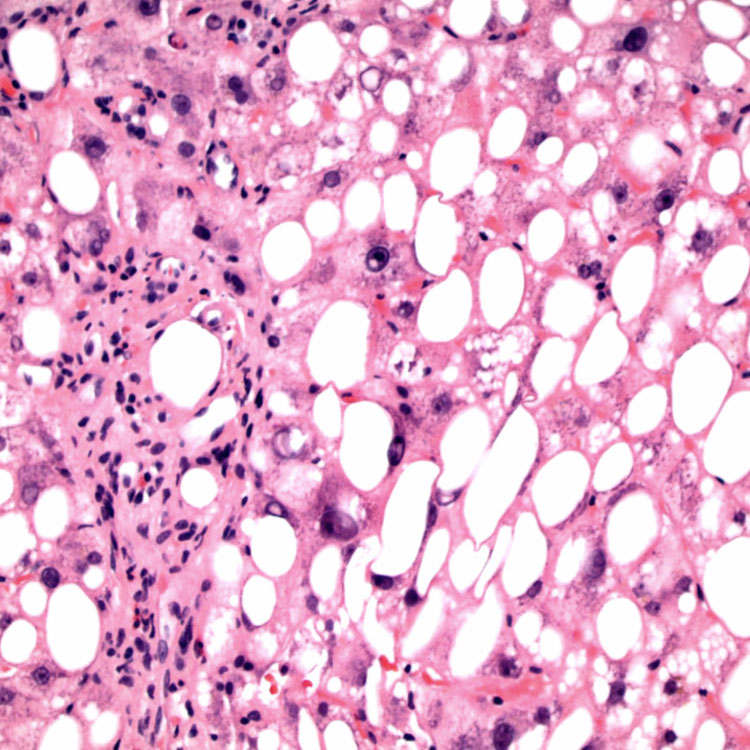
Methotrexate, Steatosis Both macrovesicular and microvesicular steatosis can be seen in methotrexate injury. Inflammation may not be prominent.
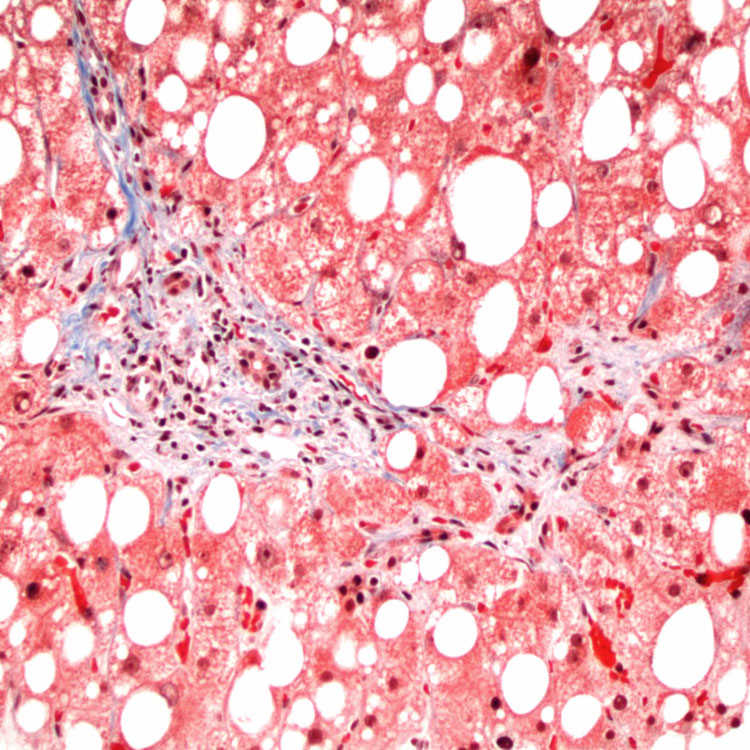
Periportal Fibrosis Trichrome stain shows delicate spurs of periportal fibrosis, as well as steatosis, in methotrexate toxicity.
TERMINOLOGY
Definitions
• Drug-induced steatohepatitis &/or phospholipidosis (intracellular accumulation of phospholipids)
Phospholipidosis likely from impaired phospholipid metabolism, although exact mechanism unknown
ETIOLOGY/PATHOGENESIS
Commonly Implicated Drugs
• Amiodarone (antiarrhythmic): Strongly tissue-bound, becomes concentrated in liver
• Nifedipine (calcium channel blocker)
• Perhexiline maleate (calcium channel blocker)
• Methotrexate (immunosuppressant/antineoplastic): Hepatic injury usually occurs after long-term use
• Tamoxifen (estrogen antagonist)
• Steroids
• Naproxen (NSAID)
• Trimethoprim-sulfa (antibiotic)
• Total parenteral nutrition
• Anti-HIV drugs
Induce syndrome of dyslipidemia, fat maldistribution, insulin resistance
– Known as HIV-associated lipodystrophy syndrome or HIV-associated metabolic and morphological abnormality syndrome (HAMMAS)












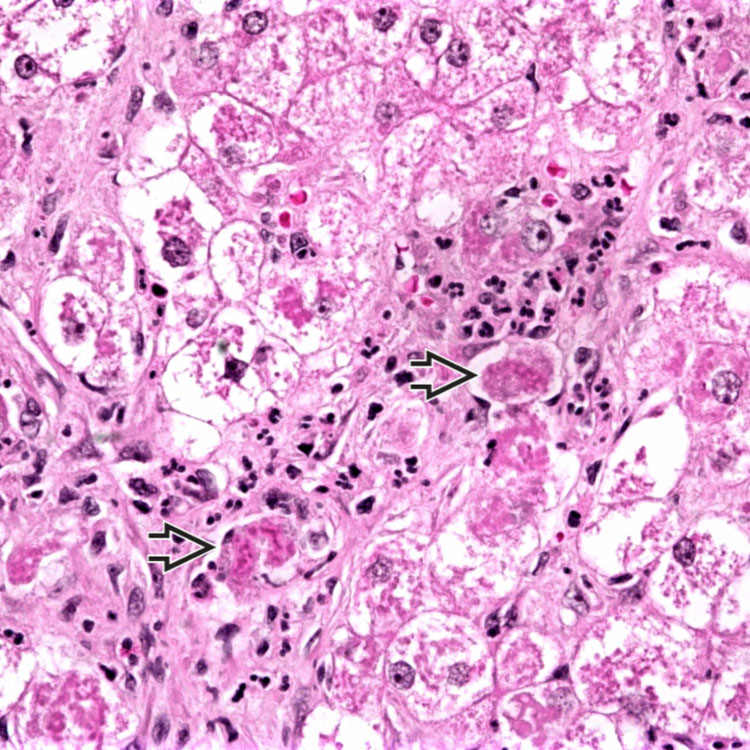
 with surrounding neutrophils (satellitosis).
with surrounding neutrophils (satellitosis).