http://evolve.elsevier.com/Edmunds/NP/
 Key drug.
Key drug.
Diuretics
The four major subclasses of diuretics—thiazides, loop, carbonic anhydrase inhibitors, and potassium-sparing diuretics (Table 32-1)—act by decreasing sodium reabsorption at different sites along the nephron. The four classes differ in terms of the specific site of action in the nephron. The ability to augment urinary losses of sodium and water is useful in the treatment of hypertension, heart failure, renal failure, and cirrhosis. A large number of thiazide diuretics are available; only the five most commonly used are discussed here. The use of potassium supplementation is discussed separately at the end of the chapter. All diuretics are now available in generic forms.

Therapeutic Overview
Sodium and chloride ions and water are freely filtered across the glomerulus. Under normal circumstances, more than 99% of these substances are reabsorbed along the renal tubule. This process requires the renal tubules to reclaim nearly 3 lb of sodium chloride each day. The reabsorption of sodium is, in general, an active transcellular process. By contrast, chloride reabsorption may be passive or active. Chloride reabsorption is most commonly coupled with sodium reabsorption, which explains the parallel reabsorption of these two ions. Water reabsorption occurs by diffusion, which is driven by solute, particularly sodium, reabsorption.
The first step of sodium and water reabsorption at each site involves the transport of sodium from the tubular lumen into tubular epithelial cells. It is this first step that is inhibited by diuretics. Each segment of the nephron contains different luminal transport proteins or channels that facilitate the entry of filtered sodium into the cell. These transport systems are inhibited predominantly by only certain types of diuretics. It is this specificity that determines the site of action of each diuretic. Once sodium has entered the tubular cells, it is pumped out of the other side of the cell by a sodium-potassium exchanger into the interstitial fluid, from which it may be returned to the circulation.
Mechanism of Action
The three major classes of diuretics (excluding combination therapy) are thiazide, loop, and potassium sparing. These are generally distinguished at the point where they impair sodium reabsorption within the renal tubule. Thiazide-type diuretics work in both the distal tubule and the connecting segment (and perhaps in the early cortical collecting tubule). Loop diuretics, the most potent, act in the thick ascending limb of the loop of Henle. Potassium-sparing diuretics work in the aldosterone-sensitive principal cells in the cortical collecting tubule.
The sites of action of the different types of diuretics are outlined in Figure 32-1 and Table 32-1. The ability of each type of diuretic to increase urinary sodium excretion depends on two factors: the amount of sodium reabsorbed at its site of action and the ability of more distal sites to reclaim that sodium. Carbonic anhydrase inhibitors act on the proximal tubule, where up to 65% of sodium is reabsorbed. However, these drugs have limited clinical usefulness as diuretics because sodium lost at this site is effectively reclaimed at more distal sites along the nephron. Loop diuretics act in the ascending limb of the loop of Henle, where 25% of sodium is normally reclaimed. Thiazide diuretics act on the distal tubule, where 3% to 5% of sodium is reclaimed. The collecting duct is the site of action of the potassium-sparing diuretics. Normally, only 1% to 2% of the sodium is reabsorbed at this site. These drugs, as their group name implies, limit urinary losses of potassium.
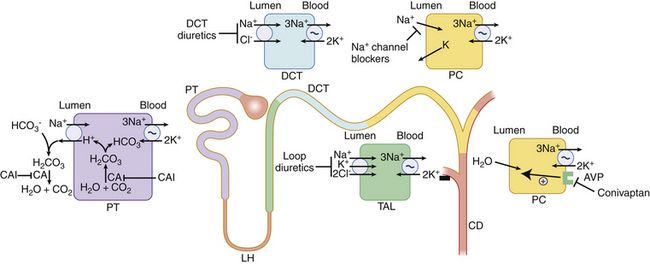
FIGURE 32-1 Sites and mechanisms of diuretic drugs.
Spironolactone (not shown) is a competitive aldosterone antagonist that acts primarily in the collecting duct. As the most distal part of the nephron, it exhibits the least amount of reabsorption. CA, Carbonic anhydrase; CAI, carbonic anhydrase inhibitor; CD, collecting duct; DCT, distal convoluted tubule; DT, distal tubule; LH, loop of Henle; PC, principal cell; PT, proximal tubule; TAL, thick ascending limb; indicates primary active transport. (From Greenberg A: Primer on Kidney Diseases, ed 5, Philadelphia, 2010, Saunders.)
Thiazide Diuretics
In all, 3% to 5% of filtered sodium is reabsorbed in the distal tubule. This reabsorption occurs via an NaCl cotransporter that is inhibited by thiazide diuretics. The therapeutic effect of this class of diuretics is partially blunted by the reabsorption of sodium that takes place distally in the cortical collecting tubule. Thus, the thiazide-type diuretics are less effective in the treatment of edema, where a large amount of fluid loss is the goal of therapy. In the treatment of patients with hypertension, however, these drugs are particularly effective because marked fluid loss is neither necessary nor desirable. The mechanisms that underlie the efficacy of thiazides in the treatment of hypertension are not completely known. Volume loss likely plays an important role. However, during long-term therapy, these drugs may act to decrease peripheral vascular resistance.
The distal renal tubule is also the primary site of calcium reabsorption. The thiazides act to enhance calcium absorption and lessen excretion. This effect is beneficial in the treatment of patients with chronic kidney stones that arise from excessive calcium excretion.
Loop Diuretics
Twenty percent of filtered sodium is reabsorbed in the loop of Henle. A cotransporter in the ascending limb of the loop of Henle and in the macula densa cells of the early distal tubule moves one molecule of sodium and potassium and two molecules of chloride from the tubular lumen into the tubular epithelial cells (see Figure 32-1). Most reabsorbed potassium then moves back out of the cell into the tubular lumen via potassium channels. Loop diuretics inhibit this cotransporter and are able to excrete up to 25% of the filtered sodium. Ototoxicity, caused by intravenous loop diuretic therapy, is thought to be related to inhibition of this cotransporter in the inner ear.
Loop diuretics promote excretion of calcium. This occurs passively as a result of sodium reabsorption inhibition. This is a clinically relevant effect in that loop diuretics and saline hydration are the treatments of choice in cases of hypercalcemia.
Carbonic Anhydrase Inhibitors
Approximately 50% to 75% of filtered sodium is reabsorbed in the proximal tubule. However, the diuretic response is generally weak because most filtered sodium is reclaimed by both the loop of Henle and the distal nephron. An important sodium transport pathway at this site is the sodium/hydrogen (sodium/H) exchanger that is located in the luminal membrane of the proximal tubular cells (see Figure 32-1). An important factor in maintenance of sodium/H exchange is the removal of hydrogen ions from the tubular lumen. If hydrogen ions accumulate, then the activity of the sodium/H exchanger is slowed. Carbonic anhydrase facilitates the removal of luminal hydrogen ions by promoting the dissociation of carbonic acid, H2CO3 (formed by the association of filtered bicarbonate with the hydrogen ions secreted into the tubular lumen by the sodium/H exchanger), to yield carbon dioxide and water. This process of carbonic acid formation and dissociation maintains low luminal hydrogen ion levels and thus allows the sodium/H exchanger to continue to reabsorb sodium. If carbonic anhydrase is inhibited, luminal hydrogen ion concentrations rise and the activity of the sodium/H exchanger is inhibited. The carbonic anhydrase inhibitors are relatively weak diuretics because of the ability of more distal sites to increase their reabsorption of sodium.
An important consequence of carbonic anhydrase inhibition is its interference with bicarbonate reabsorption (see Figure 32-1). The distal nephron sites are not able to reclaim all of this additional bicarbonate; as a result, bicarbonate is lost into the urine. This loss of bicarbonate can be an advantage in the treatment of individuals with severe metabolic alkalosis, in whom this bicarbonate loss can limit alkalemia. However, loss of urinary bicarbonate can also lead to severe metabolic acidosis.
Potassium-Sparing Diuretics
The collecting duct plays a major role in the day-to-day regulation of NaCl and potassium excretion. Sodium reabsorption along this segment, which reabsorbs only 3% to 5% of filtered sodium, occurs via a luminal sodium channel. The reabsorption of sodium generates a voltage gradient that drives potassium from the tubular cell into the tubular lumen and hence into the urine. Blocking of sodium reabsorption at this site slows potassium excretion and leads to the potassium retention for which diuretics that act on this segment are named. The net diuretic effect is approximately 1% to 2% filtered sodium. These diuretics are commonly paired with a loop or a thiazide for refractory edema or to blunt potassium loss.
Aldosterone Antagonists
Tubular epithelial cells in the collecting duct possess high-affinity receptors for the hormone aldosterone. Occupancy of these receptors by aldosterone initiates a number of events, including activation of previously inactive luminal sodium channels, transport of additional sodium channels from the cytosol to the luminal cell membrane, and stimulation of the production of other sodium channels. Spironolactone and eplerenone competitively inhibit the aldosterone receptor. Eplerenone differs from spironolactone in that it is a more specific inhibitor of aldosterone and produces fewer endocrine side effects. The net diuretic effect of the aldosterone antagonists is approximately 1% to 2% filtered sodium. However, these drugs are particularly useful in the treatment of cirrhosis and ascites and have been shown to improve survival in patients with advanced heart failure.
Treatment Principles
Evidence-Based Recommendations
Refer to Chapters 17 and 19 for recommendations in the treatment of hypertension and heart failure.
Cardinal Points of Treatment
These treatment options may vary if the patient has renal insufficiency.
Pharmacologic Treatment
An important factor in diuretic efficacy is the patient’s ability to adhere to a low-sodium diet. As drug concentration falls, a period of positive sodium balance—the period of postdiuretic sodium retention—may follow. If dietary salt intake is high, then the amount of sodium lost in response to the diuretic may be partially or completely offset by postdiuretic sodium retention.
Renal function is another important variable in determination of diuretic response. Patients become less responsive to diuretics as renal function declines. Loop diuretics typically retain efficacy even in the face of moderately severe renal insufficiency; however, patients may require higher diuretic doses to achieve an effect. Most thiazides are relatively ineffective in individuals with a glomerular filtration rate (GFR) <30 ml/min. Exceptions to this are metolazone and indapamide. Potassium-sparing diuretics should be used with great caution or should be avoided in patients with renal insufficiency because of their potential to induce life-threatening hyperkalemia.
In addition, length of time on therapy may contribute significantly to the responsiveness of the kidneys to diuretics. The ability of a diuretic to increase renal NaCl excretion declines over time. This phenomenon, referred to as diuretic resistance, is thought to occur in one of every three patients with heart failure (HF). A second drug that is added may act synergistically to mitigate this adaptive process.
For diuretic resistance, evaluate and treat these factors: patient nonadherence (either not taking drug or high NaCl intake), HF, renal failure, increased renal insufficiency, nephrotic syndrome, and cirrhosis. Drugs that may cause diuretic resistance include NSAIDs, captopril, cimetidine, and some antihypertensives. (See Boxes 32-1 and 32-2.)
The loop diuretics, thiazide diuretics, and carbonic anhydrase inhibitors are sulfonamide derivatives, and the provider should pay close attention to the specific reaction of a patient who reports an allergy to a sulfonamide or a “sulfa” drug (e.g., Bactrim, Septra, generic) because individuals with sulfa allergies often have a predisposition to allergic reactions in general, as opposed to cross-reactivity with sulfonamide drugs. The nonsulfonamide loop diuretic ethacrynic acid is reserved for the patient who develops a true allergic reaction to a loop or thiazide diuretic.
As with any medication, it is important for the clinician to determine the patient’s previous response to treatment and history of any adverse events. Additional considerations include cost, mobility, and toileting concerns that may affect a patient’s adherence to prescribed diuretic therapy.
Thiazides
Thiazides are the most frequently used and least expensive antihypertensive drugs. Early studies clearly demonstrated blood pressure reduction; however, metabolic effects such as hypokalemia, hyperuricemia, and hyperglycemia were seen. Even more important, demonstration of a significant reduction in coronary events following BP reduction was difficult, and this limited their widespread use. Dosages of hydrochlorothiazide in these early studies were in excess of 50 mg per day. In later studies, doses greater than 25 mg per day were shown to limit the extent of these metabolic effects while reducing blood pressure. These findings led to initiation of the Antihypertensive and Lipid-Lowering treatment to prevent Heart Attack Trial (ALLHAT).
ALLHAT, the largest prospective study on hypertension to date, compared the efficacy of an angiotensin-converting enzyme inhibitor (lisinopril, 10 to 40 mg per day) or a calcium channel blocker (amlodipine, 2.5 to 10 mg per day) or doxazosin (an α-adrenergic blocker) vs. a thiazide diuretic (chlorthalidone, 12.5 to 25 mg per day) in preventing major outcomes in high-risk hypertensive patients. More than 33,000 patients were enrolled in the study from 1994 to 2002 and were followed for a mean of 5 years. Patients were 55 years of age or older with a diagnosis of hypertension and at least one risk factor for coronary heart disease (CHD). The doxazosin arm was prematurely stopped during an interim analysis that showed an increased risk of heart failure (8.1% vs. 4.5% at 4 years) compared with chlorthalidone.
At the end of the study, all three drugs were noted to be effective in reducing blood pressure and providing protection from CHD and nonfatal myocardial infarction. However, chlorthalidone was shown to be superior to the other drugs in terms of the following outcomes.
Compared with chlorthalidone, lisinopril had higher rates of the following:
Compared with chlorthalidone, amlodipine had a higher rate of the following:
The benefits of chlorthalidone treatment in ALLHAT were evident in men, women, African Americans, non–African Americans, those with and without diabetes, and younger and older patients. Adverse effects, specifically hypokalemia and hyperglycemia, were more frequent in the chlorthalidone group. Hypokalemia occurred in 8.5% vs. 1.9% and 0.8% in the amlodipine and lisinopril groups, respectively. Potassium supplementation, as expected, was more frequent in the chlorthalidone group and was required in 8% of patients. A fasting blood sugar >126 mg/dl was also seen in 11.6% of patients receiving chlorthalidone among those without diabetes. This was more frequent than in those receiving amlodipine (9.8%) and lisinopril (8.1%).
Based on results from the ALLHAT trial, the seventh Joint National Committee (JNC 7) report recommended that a thiazide diuretic be given as initial treatment of hypertension unless a specific indication for a drug from another class is noted. The authors also believed that the benefits of chlorthalidone would be translated to hydrochlorothiazide at similar doses of 12.5 to 25 mg once daily, but this recommendation is not evidence-based.
The addition of a thiazide to a loop diuretic and sodium restriction may be useful in the treatment of refractory edema in patients with CHF, cirrhosis, nephrotic syndrome, and renal failure. The rationale for this combination involves inhibition of sodium reabsorption at multiple sites along the nephron and the fact that in CHF, most patients have altered creatinine clearance, so loop diuretics are more effective.
Thiazides are useful in reducing the frequency of new stone formation in patients with idiopathic hypercalciuria because of their ability to decrease renal calcium excretion. This enhanced calcium excretion results in a positive calcium balance that may reduce the number of fractures in older patients. An analysis of 18 observational studies of more than 29,000 patients revealed that the use of a thiazide diuretic on a long-term basis may reduce osteoporotic fractures by up to 20%. The same is not true of loop diuretics because these drugs produce a negative calcium balance and have been shown to increase the risk of hip fracture associated with osteoporosis.
Thiazides also may be used to decrease urine volume in patients with nephrogenic diabetes insipidus. Thiazide diuretics given in combination with a low-salt diet in the management of Ménière’s disease may decrease the natural progression of sensorineural hearing loss and may be used to treat vertigo through prevention of flare-ups.
As is the case with most diuretics, major complications of thiazide therapy include fluid and electrolyte abnormalities. Of concern is the increased incidence of sudden death seen in early studies with doses >50 mg per day in patients with hypertension. However, the ALLHAT trial clearly showed that this finding was dose related.
As a general recommendation, thiazides should be started at the lowest dosage, and those with shorter half-lives should be given once or twice daily. Doses no greater than 25 mg daily of hydrochlorothiazide or chlorthalidone should be given for the treatment of hypertension; the adverse effects of hypokalemia, hypomagnesemia, and increased cholesterol, as well as a possible increase in sudden death, among thiazide-treated patients appear to be dose related.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


