Chapter 15 Diuretics
3. It plays a fundamental role in maintaining pH, controlling levels of electrolytes and water, and conserving substances such as glucose and amino acids.
a. Blood is forced into the glomerulus and filtered through capillaries into the glomerular capsule.
c. Substances normally not filtered include cells, plasma proteins and substances bound to them, lipids, and other macromolecules.
b. Many drugs are actively secreted by anion (e.g., penicillins and most other β-lactam drugs, glucuronide conjugates of drugs) or cation (e.g., protonated forms of weak bases and quaternary ammonium compounds) transport systems.
c. Probenecid blocks anion transport and N-methylnicotinamide blocks cation transport in the kidney.

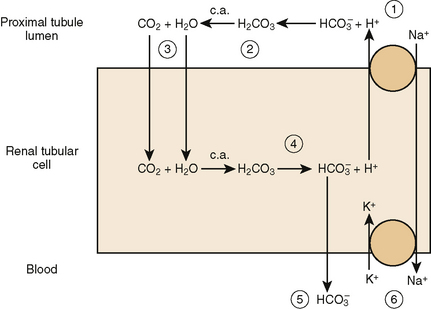
a. Carbonic anhydrase is located in the brush border and cytosol of the proximal renal tubule (PRT) cells.
(2) H+ ions combine with filtered bicarbonate in the brush border of the PRT to produce carbonic acid (H2CO3; step 2).
(3) Carbonic anhydrase (c.a.) in the brush border dissociates H2CO3 to CO2 and water, which are reabsorbed into the PRT (step 3).
(5) Bicarbonate is reabsorbed into the blood and H+ ions are exchanged for filtered sodium to repeat the cycle (step 5).
b. Carbonic anhydrase inhibitors decrease the sodium/H+ exchange by decreasing H+ production in the PRT.
c. This changes the composition of urine by increasing bicarbonate, sodium, and potassium excretion (this effect lasts only 3 to 4 days).
d. Increased loss of bicarbonate alkalinizes the urine and produces a mild hyperchloremic normal anion gap metabolic acidosis (type II proximal renal tubular acidosis)
• Carbonic anhydrase inhibitors decreases production of aqueous humor; hence, lowering intraocular pressure.
b. Loop diuretics cause a profound diuresis (much greater than that produced by thiazides) and a decreased preload to the heart.
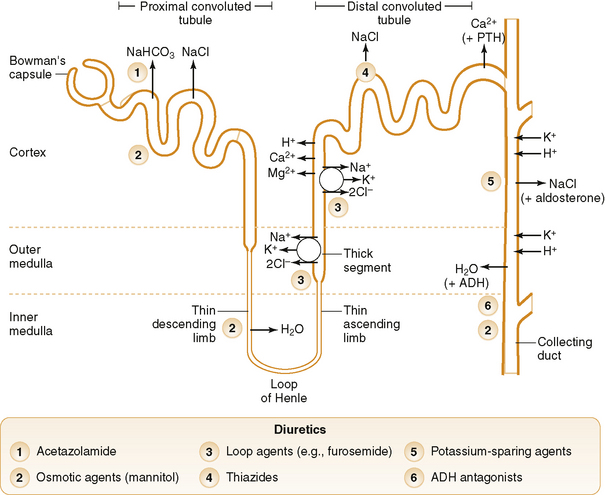
c. These drugs inhibit reabsorption of sodium and chloride in the thick ascending limb in the medullary segment of the loop of Henle (Fig. 15-3)
(1) Increase excretion of obligated water (water attached to sodium, potassium, etc.), sodium, chloride, magnesium, and calcium (step 1)
d. These drugs are useful in patients with renal impairment because they retain their effectiveness when creatinine clearance is less than 30 mL/min (normal is 120 mL/min).
e. Loop diuretics up-regulate cyclooxygenase activity, thereby increasing prostaglandin E2 (PGE2) and prostaglandin I2 (PGI2) synthesis, resulting in increased renal blood flow.
• Inhibition of a sulfhydryl-catalyzed enzyme system that is responsible for reabsorption of sodium and chloride in the proximal and distal tubules.
(1) In patients who are hypersensitive to sulfonamide drugs such as thiazides and furosemide (the most commonly used loop diuretic)
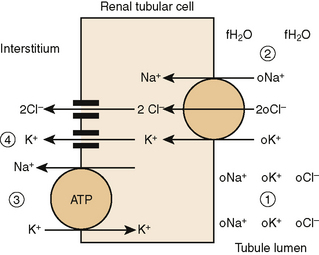
• Inhibition of reabsorption of sodium and chloride by attaching to the chloride-binding site of the Na+/K+/2Cl− (NKCC2) cotransporter in the thick ascending limb in the medullary segment of the loop of Henle
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


