Associated with low recurrence and metastatic rates
Microscopic
• Multinodular solid or cystic tumor based in dermis
• Solid areas composed of dense collections of cells with focal ductal lumina
• Cystic/glandular areas with papillary projections often seen (although may be focal or absent in some cases)
• Mitotic figures often seen; can be numerous
• Focal necrosis may be present
Top Differential Diagnoses
• Eccrine carcinoma
Head and neck location
More infiltrative, small cords and nests of basophilic cells
• Apocrine carcinoma
Axillary and groin locations
Infiltrative lobules, nests, and cords of eosinophilic-staining cells
• Apocrine adenoma
• Spiradenoma
• Cylindroma
Digital Papillary Adenocarcinoma Digital papillary adenocarcinoma shows a nodular, basaloid tumor in the mid to deep dermis. Although the tumor is relatively well-circumscribed in most areas , there are other areas that appear more infiltrative .
Intermediate Magnification of Nodular Area This nodular area is composed of crowded basaloid cells forming irregular cords and focal ductal lumina . There is surrounding stromal sclerosis and inflammation .
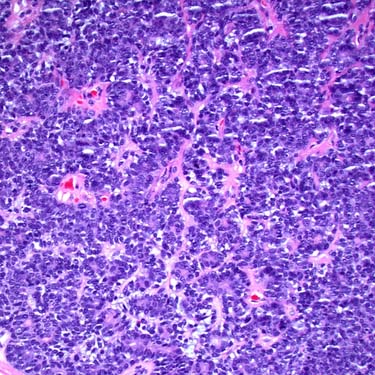
High Magnification of Cellular Area This more cellular area is composed of irregular, anastomosing cords of crowded basaloid cells showing nuclear hyperchromasia.
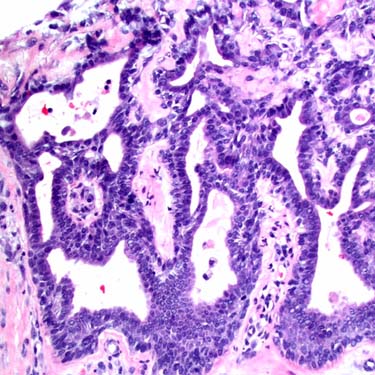
High Magnification of Glandular Area This focus is composed of irregular, anastomosing glandular structures lined by cuboidal epithelial cells. Although the cells are small and relatively bland appearing, they show nuclear crowding and hyperchromasia.
TERMINOLOGY
Abbreviations
• Digital papillary adenocarcinoma (DPA)
Synonyms
• Aggressive DPA
• Aggressive digital papillary adenoma (misnomer, as all are considered malignant)
Definitions
• Malignant sweat gland tumor that typically presents on digits of young adult patients
ETIOLOGY/PATHOGENESIS
Unknown
• May be associated with solar damage
• One case possibly associated with HPV infection
CLINICAL ISSUES
Epidemiology
• Incidence
Rare tumors
• Age
Young to middle-aged adults (mean age: 43 years)
– Some cases also reported in children
• Sex
Most cases occur in men
Presentation
• Papular or nodular lesion on digit
Typically present on distal finger (most commonly) or toe but some cases on proximal digit/webspace
Often slowly growing and painless (leading to delayed diagnosis)
Treatment
• Complete and wide excision or amputation
• Sentinel lymph node biopsy has been advocated, given significant incidence of metastasis
However, most metastases involve lungs
Prognosis
• Wide excision or amputation associated with low recurrence and metastatic rates
However, some cases present with metastatic disease
Metastatic disease can also develop years after initial diagnosis, so long-term follow-up required
MACROSCOPIC
General Features
• Dermal nodular or nodular-cystic lesion
Only gold members can continue reading. Log In or Register to continue




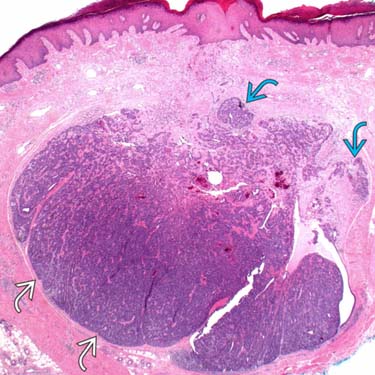
 , there are other areas that appear more infiltrative
, there are other areas that appear more infiltrative  .
.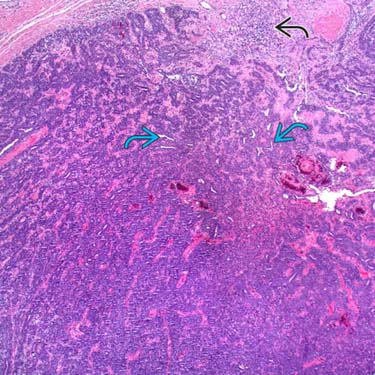
 . There is surrounding stromal sclerosis and inflammation
. There is surrounding stromal sclerosis and inflammation  .
.