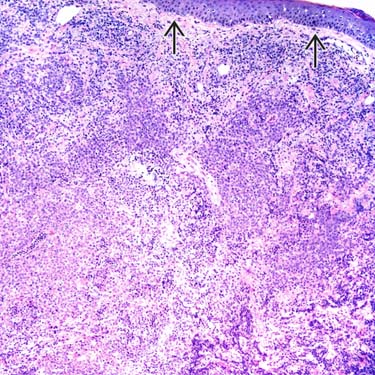
Morphologic Features of PCDLBCL-LT Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT) shows a diffuse infiltrate replacing the dermis with sparing of the epidermis .
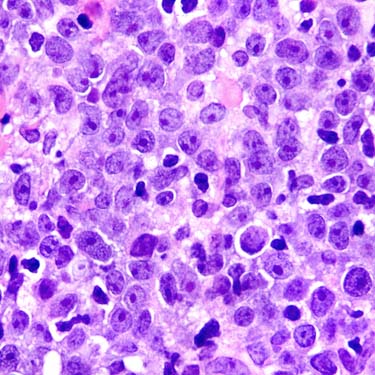
Morphologic Features of PCDLBCL-LT The lymphoma cells in PCDLBCL-LT are large and strikingly round with centrally located nucleoli (immunoblasts).
CD20 IHC in PCDLBCL-LT In this case of PCDLBCL-LT, the lymphoma cells are strongly CD20(+) and form cohesive-appearing sheets. The epidermis is not involved, and a thin grenz zone is present .
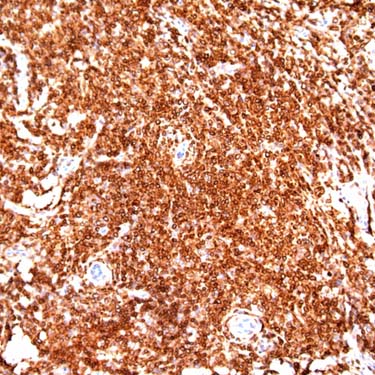
Bcl-2 Staining in PCDLBCL-LT Most cases of PCDLBCL-LT are strongly and diffusely Bcl-2(+), as shown in this case.
TERMINOLOGY
Abbreviations
• Primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT)
Synonyms
• Primary cutaneous large B-cell lymphoma, leg type
• Primary cutaneous diffuse large B-cell lymphoma
Definitions
• Primary cutaneous diffuse large B-cell lymphoma composed exclusively of large transformed B cells
Often occurs in lower leg(s) but can arise at other sites
ETIOLOGY/PATHOGENESIS
Cell of Origin
• Peripheral B cell of postgerminal center cell origin
Immunophenotype: IRF-4/MUM1(+), FOXP1(+)
High frequency of somatic mutations of IGH variable (V)-region genes
Possible Role of Antigen Selection
• Preferential use of certain IGH (IGHV) gene segments
Suggests that antigen stimulation may be involved in pathogenesis
Role of Molecular Abnormalities
• Number of genetic rearrangements and deletions reported
• No abnormality consistently present
CLINICAL ISSUES
Epidemiology
• Incidence
Rare
– 4% of all cutaneous lymphomas
– 20% of primary cutaneous B-cell lymphomas
• Age
Elderly patients; median age: 7th decade
• Sex
More common in women
– M:F ratio: 1:1.6; as high as 1:4 in some studies
Site
• Most cases arise in skin of lower leg(s): 1 or both legs may be involved
~ 85% of all cases
• Subset of cases arise in skin of other sites (trunk, arms, head and neck)
~ 15% of cases
Similar morphologic and immunophenotypic characteristics
• Single or multiple lesions at time of presentation
Some patients have dissemination at initial diagnosis
Presentation
• Red or blue-red cutaneous lesions
Plaque, verrucous plaques, or deep plaques
Nodular, tumoral lesions
Often associated with ulceration
Multiple lesions are common
• B symptoms in 10-20% of patients
Treatment
• Anthracycline-containing systemic chemotherapy plus rituximab
• Radiotherapy has role for localized lesions in elderly patients
Prognosis
• Relapse is common
• 40-50% 5-year survival rate
Factors adversely correlated with prognosis
– Older age
– Multiple lesions at presentation
– Inactivation of CDKN2A
Factors not correlated with prognosis
– Duration of lesions before diagnosis
– Gender, B symptoms, performance status, or serum lactate dehydrogenase level
– Bcl-2 or IRF-4/MUM1 expression
MICROSCOPIC
Histologic Features
• Diffuse pattern of involvement of dermis
Infiltrate can be deep, often extending into superficial subcutaneous adipose tissue
• Cohesive, monotonous sheets of atypical-appearing large cells
Centroblasts or immunoblasts
Often very round nuclei; can also be oval
• Mitotic figures numerous
• Few small reactive T cells in background
• No centrocytes (or small B cells) present
• No epidermotropism
ANCILLARY TESTS
Immunohistochemistry
• Pan-B-cell antigens (+)
• Cytoplasmic IgM(+), IgD(+/-)
• Bcl-2(+), IRF-4/MUM1(+), FOXP1(+)
• Bcl-6(+), CD10(-)
• No follicular dendritic cell (FDC) meshworks
CD21(-), CD23(-), CD35(-)
• T-cell antigens (-), LMP1(-), HHV8(-)
In Situ Hybridization
• FISH often shows rearrangements of MYC, BCL6, or IGH genes
No evidence of IGH-BCL2 /t(14;18) or BCL2 rearrangements
Only gold members can continue reading. Log In or Register to continue



 .
.
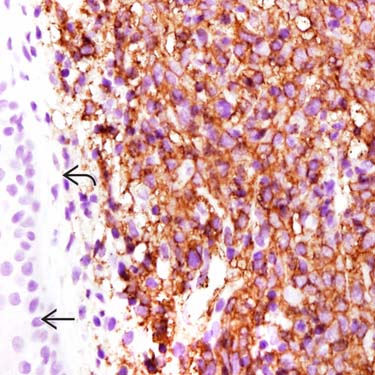
 is not involved, and a thin grenz zone is present
is not involved, and a thin grenz zone is present  .
.